Fundamental to anti-oppressive social work praxis—the act of enacting, implementing or applying a form of practice—within Indigenous communities is to incorporate and implement a decolonized, trauma-informed, and culturally-safe framework. At the core of these frameworks are relationality and relational accountability. Throughout this chapter I will speak to praxis, rather than practice, as praxis is the intentional enactment of the frameworks (practice). An essential foundation of a dynamic social work praxis is to build relationships within Indigenous communities and with community members, while valuing and implementing the knowledge systems and values therein. As Indigenous or non-Indigenous social workers, the social work profession must examine how it has been colonially developed, and often maintains settler-colonial policy and practices; this approach devalues Indigenous sacredness of relationships. Comprehension of the historical manifestation of social work is imperative to prevent perpetuating colonial harm, alongside understanding the effects of colonization in rural and remote Indigenous communities. The views shared throughout this chapter must not be interpreted as a concrete blueprint for working within these communities, but rather, to underscore the importance of relationality with community and community members in social work practice.
The purpose of this chapter is to critically examine the history of social work in its relation to settler-colonial policies, to understand how our individual education, beliefs and worldviews may be informed by settler colonialism. While evaluating history, structures, and policies, we can critically examine our roles as social workers within rural and remote Indigenous communities, strive to develop meaningful relationships, and to integrate and establish our roles as helpers or co-creators, rather than as saviours.
The discussion of social work history and current policies can produce feelings of shame and discomfort. It is important to acknowledge these feelings, while working to understand the roots of these feelings, rather than resorting to offence and/or disregard. It is through this personal work that social workers can become co-creators, helpers, and allies.
The first part of this chapter will examine the history of settler colonialism and its roots within social work practice. Examining the roots of social work will provide context to understanding current and intergenerational trauma within Indigenous communities. Next, social work praxis will be explained through the importance of enacting an anti-oppressive practice, building relationships within community, cultural safety, decolonial praxis, and trauma-informed practice. The chapter will conclude with an explanation service delivery and connections to incorporating the Truth and Reconciliation Commission of Canada (TRC) and the United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP) into practice.
Learning Objectives
By the end of this chapter you will have had the opportunity to:
- Understand the history of social work on Turtle Island (North America) and its current impact and implications within Indigenous communities;
- Evaluate our systems of knowledge, values, and experiences that form our own belief systems, including the ways that our settler worldviews impact our work in community;
- Understand the importance of relationships and relationality with and within community; and
- Understand anti-oppressive practice in order to actively implement culturally safe, decolonized, and trauma informed practice within rural and remote Indigenous communities.
History of Settler Colonialism in Social Work
To comprehend and contextualize social work praxis, the history of colonial, oppressive and assimilative policies that were implemented and carried out by social workers must be evaluated. Historically, settler-colonial ideology disregarded Indigenous ways of being and knowing, and legally prohibited Indigenous structures and living, such as hunting and gathering, family and community, governance, knowledge systems, spirituality and culture. Settler colonialism is different from other forms of colonialism, because it includes taking control of the land and all things in its domain (Tuck & Yang, 2012). Social workers were an essential element of the ongoing “assimilative policy projects” implemented by the government, which attempted to destroy Indigenous identities, families, communities, relationships, languages, and knowledge systems (Hart et al., 2010, p. 20), and carried out actions to maintain social control (Pugh & Cheers, 2010).
In the context of micro, mezzo and macro practice, many Indigenous worldviews identify that systems of individual, community, and nation are inseparable, and are interrelated within the understanding of wellbeing and kinship. Policies, legislation, and legally-binding documents were established, such as the treaties, the Constitution Act (1867), and the Indian Act (1876), to dismantle and extinguish Indigenous identities (micro), families and communities (mezzo), and Indigenous structures, systems, and governance (macro) (Greenwood et al., 2017).
The attempt to extinguish Indigenous identity (micro) included prohibiting spiritual and cultural practices, speaking Indigenous languages (such as within the Indian Residential School (IRS) system), and changing Indigenous names to more white-colonizer sounding names through treaties and residential schools, as residential “schools were attempting to make “little white children out of little red children”.” (Aboriginal Healing Foundation, 2006, p. 2). Settler-colonial ideologies of a superior race (white), or the notion to “kill the Indian in him, and save the man” (Pratt, 1892), have profound effects on Indigenous identity, which can lead to internalized colonialism (Bleau & Dhanoa, 2021). Internalized colonialism and denying Indigeneity, or ties to Indigenous background, can be maintained intergenerationally through family as a protection from alienation and ostracism from mainstream society.
Family and community systems (mezzo) were broken and legally separated through forced assimilation, including mandatory attendance at Indian Residential Schools (IRS), and the forced removal of children from their families, and illegal adoptions, during the Sixties Scoop. It was believed that removing Indigenous children from their families would rid Indigenous communities of their traditional ways and languages—referred to as “savage”—in order to assimilate Indigenous children into a “higher race” of the “English-speaking and civilized” (Official Report of the Nineteenth Annual Conference of Charities and Correction, 1892). Approximately 150,000 children attended Indian Residential Schools (IRS) from 1870 through the 1990s (Walker, 2015). In 1892, Richard H. Pratt, founder and superintendent of the Carlisle Indian Industrial School, stated:
A great general has said that the only good Indian is a dead one, and that high sanction of his destruction has been an enormous factor in promoting Indian massacres. In a sense, I agree with the sentiment, but only in this: that all the Indian there is in the race should be dead. Kill the Indian in him, and save the man. (Official Report of the Nineteenth Annual Conference of Charities and Correction, 1892)
Pratt’s ideology fueled the disregard for Indigenous life. The death rate of Indigenous children in Residential Schools itself is considered an act of genocide, with some schools having a death rate of 40% (Truth Commission into Genocide in Canada, 2001). Indian Hospitals targeted individuals and performed illegal / abusive medical procedures, including sterilization of women and girls, often without pain medication (Truth Commission into Genocide in Canada, 2001).
Under the Indian Act (1876) Indigenous systems (macro) were dismissed or legally prohibited, such as systems of governance, cultures, and ceremonies, and the forced and mandatory relocation to reserves. Some policies could be considered imprisonment, such as the Pass System, which prohibited Indigenous individuals from leaving the reservation without a legal “pass” from an Indian agent (Johnson, 2020). Individuals could be incarcerated for leaving reservations, even for survival purposes, such as hunting, fishing and gathering, or visiting with relatives (Johnson, 2020). Reservations could be viewed as mass prisons, which were controlled through Indian Agent surveillance.
The settler colonialism that occurred within Turtle Island (North America) was genocide, resulting in the extinction of over 90% of some populations (Greenwood et al., 2017). Indigenous people were viewed as unworthy of occupying space, as Pratt states “they occupy so much more space than they are entitled to either by numbers or worth” (Official Report of the Nineteenth Annual Conference of Charities and Correction, 1892). Indigenous people were viewed as weak by colonizers, and it was assumed that Indigenous people would become extinct or fully assimilated (Greenwood et al., 2017; Tuck & Yang, 2012).
Greenwood et al. (2017) state that colonizers viewed Indigenous people as inherently weak and prone to sickness and therefore policies were implemented to reflect a paternalistic “protection.” Robidoux and Mason (2017) assert that settler-colonial control was justified by colonizers, because the ideology of success was associated with mass production, profit, and thus power. Indigenous ways of being and living, such as communal hunting, fishing, gathering, and equitable sharing lacked the basis of mass agricultural production and did not conform to the principles of capitalism. Pratt stated that he believed Indigenous people lacked the ability to exploit the land for their own use, which he viewed as foolish (Official Report of the Nineteenth Annual Conference of Charities and Correction, 1892). For this reason, Indigenous ways of living were not highly valued, and thus directed by settler-colonial policies; Indigenous Nations were forced to farm, rather than to hunt and gather.
Indigenous people were robbed of their Indigeneity, land, culture, traditions, language and kinships in the name of colonialism and capitalism. These injustices stripped Indigenous peoples of the ability to exercise their autonomy to suit their own needs and interests (UNDRIP, 2008).
Settler Colonialism roots in Social Work
Social workers have been historically complicit in the unjust treatment of Indigenous people, as they played an active role in the kidnapping of Indigenous children for both Indian Residential Schools (IRS) and the Sixties Scoop. Social workers accompanied Royal Canadian Mounted Police (RCMP) officers to seize Indigenous children from their families. This act of illegally displacing Indigenous children continued into the era of the Sixties Scoop, where Indigenous children were fostered by, or adopted into, non-Indigenous families. As viewed through settler-colonial ideologies, which formed the profession of social work, Indigenous people and families were perceived as a “problem,” who could be “saved” from their “dysfunctional” selves, families, and communities (Australian Human Rights Commission, 2001). Indigenous people were also viewed as “savages” who were captive to their nation’s / tribe’s “savage language, superstition, and life” (Official Report of the Nineteenth Annual Conference of Charities and Correction, 1892).
Assimilation policies and colonial violence have led to a widespread Indigenous distrust of the government and those who occupy “white” government agencies (Pugh & Cheers, 2010). The historical policies and proceedings continue to carry deeply ingrained colonial and systematic forms of oppression which have continued the displacement of children into child welfare systems—constructing a pipeline to prison—and exacerbated psychological trauma and physical illness (Hart et. al., 2010; Johnson, 2020; TRC, 2015).
Fortier and Wong (2018) state that social work and the implementation of social services has “been created out of the trauma of dispossession,” which discounts Indigenous systems and knowledges and instead “work[s] with the more muted goals of alleviating the worst suffering while consciously or unconsciously supporting the ongoing process of dispossession” (p. 444). Thomas and Green (2020) encourage us to ask ourselves, as social workers, how historical oppression, assimilation and genocide contributes to community members’ perceptions of, and comfort with, social workers. They note that if a social worker were to ask an Indigenous community member or a family, “What is a social worker?” and “How would your ancestor answer this question?” (Thomas & Green, 2020, p. 92), the response might be shaped by personal worldviews and historical betrayal. We must recognize how and why social work was implemented in Indigenous communities, embodied as saviourism, in order to dismantle and deconstruct our understandings of social work with Indigenous people and within Indigenous communities. Once this is recognized, we can then re-create our roles as helpers and healers in community.
Rural and Remote Indigenous Community Practice
Rural and remote communities lie outside cities, and often have less access to resources and services, such as those associated with health and education. Rural communities are defined as having a population of fewer than 1,000 people living outside urban areas (Statistics Canada, 2018). Rural has been described as a physical place, climate, and economy; its resulting social context is regarded as remote or isolated, with sparse populations and limited services (Pugh & Cheers, 2010; Schmidt, 2010). However, Martinez-Brawley (2000) has recommended referring to these areas as “small communities” rather than specifically defining and labeling these areas as rural.
Collier (1984; 1993; 2006) states that “rural” is colonially defined, and has been used to name the places that Indigenous people occupy, which are often less valued spaces. Specifically for Indigenous people, the concept has been developed and based on settler-colonial standards and decisions of forceful creation of space, borders and determining resources (Pugh & Cheers, 2010; Schmidt, 2010). Rural areas that Indigenous people occupy, such as reserves which account for approximately 0.2 – 0.4 percent of land in Canada, are often utilized for resource extraction, such as through placing pipelines, that have adverse effects on health and wellbeing (Joseph, 2018; Kestler-D’Amours & O’Toole, 2019).
The lack of community resources for coping with these adverse health effects on rural communities will be discussed later in this chapter. Pugh and Cheers (2010), and Schmidt (2010) define rural as an understanding of the lack of resources available in that community. Lack of resources that are often available within cities or urban areas, may include health care (hospitals, nurses and doctors), education, mental health supports and services, substance use and harm reduction services, courts or probation offices, offices for social development (license, identification, health care documentation), grocery stores, and more.
Comprehending rural social work praxis through an anti-oppressive practice lens also includes understanding how rurality has been created and defined. Schmidt (2010) refers to Collier (1984; 1993; 2006) when speaking about the history of social work, stating that social work functioned to moderate capitalism and preserve the status quo by maintaining a certain dynamic of power and control within rural communities. Social workers must understand the current realities and inequities found in rural areas and small communities by knowing that these communities are a product of settler colonialism through exploitation and underdevelopment, leading to the elitism of settlers (Zapf, 1985). Elitism was created by utilizing government entities, such as Indian agents, and later, social workers, to direct Indigenous people and restrict them. For example, government administrations intentionally restricted Indigenous people’s access to food, such as attempting to eliminate the buffalo, followed by implementing government “policies that ensured failure rather than encouraged success” (Bateman, 1996, p. 12). Indigenous people were forced to live on reservations, which were intentionally placed on lands that were deemed unsuitable for sustainable farming (Bateman, 1996). Inadequate farming equipment was distributed to Indigenous people, compared to that of the neighbouring settlers, who were actually allotted land well-suited for farming (Bateman, 1996).
Social workers historically preserved elitism, by:
Promoting the potential development of one set of people at the expense of another set of people (elitism); that suggest that one set of people have greater human potential than another set of people (gender, racial inequality) or that deny that one or more set of people have human potential (oppression, slavery). (Delaney, 2009, p. 18).
The continuation of “relief” food was preserved through the work of social workers, continuing restrictive practices and promoting dependence on the government rather than encouraging sustainability and community development (Fortier & Wong, 2018).
Social Work in Rural and Remote Communities
Instead of replicating social work practice and service patterns that are common within other geographical areas, such as cities and urban areas, social workers must consider the history of ruralism and the unique needs of these communities (Pugh & Cheers, 2010). This shift can be achieved through both a culturally-safe framework and a generalist social work practice approach. Generalist social work practice involves remaining “skilled in working with individuals, families, small groups, organizations and communities” (Locke & Winship, 2005, p. 6) while also having a role as a resource navigator. For example, to combat the lack of resources, some Indigenous communities in British Columbia have resourced groups, such as Wellbriety, which deliver group counselling sessions while also integrating capacity building and resource navigation, such as equipping community members with harm reduction training and supplies. Other resource navigation approaches involve advocating for community members to have equitable access to resources, through video or Telehealth calls to health care workers such as nurses, doctors, psychiatrists, or courts and probation services.
A generalist practice approach is helpful within rural areas or small communities because social workers have many roles, which requires the ability to be multifaceted or versatile in order to meet the needs of the community member. As a social work colleague stated to me: “We work with whatever needs people have when they walk through the door” rather than engaging in a singular role (J. Kent, personal communication, February 2019). In restricting social work to a singular, specialized role or approach within rural communities, community members’ needs are not met. For example, some rural communities lack specific A&D workers (alcohol and drug workers). A social worker may not have the precise skillset or knowledge to complete addictions treatment applications with a client but is still considered “qualified” to fill that role. It is important to be adaptable and “general” or broad in being flexible in learning various skillsets or applications/assessments, so that community members are able to access appropriate services.
Anti-Oppressive Education & Practice
Rural Indigenous communities, which include reservations, were created to control, segregate, displace and oppress Indigenous people. Anti-oppressive practice acknowledges the historical injustices that have occurred, and actively works to prevent further harms from occurring. This section reviews historical forms of oppression, while evaluating how education is often dominated by settler-colonial views. It also explores fundamental elements of anti-oppressive practice, including the role of building relationships, cultural safety, decolonial praxis and trauma-informed practice. It is imperative to understand the importance of these unique practices, as they all uphold anti-oppressive values. Anti-oppressive practice is achieved by listening to, and implementing, the ways in which individuals and communities envision their healing, without overriding their decisions with one’s own personal biases or worldviews. Part of this process is to implement Two-eyed Seeing (Western and Indigenous healing methods and ideologies), rather than strictly encouraging colonial therapies and pathologizing, or “diagnosing” Indigenous experiences. Two-eyed Seeing incorporates both Indigenous and settler-colonial knowledge. Greenwood et al. (2017) describe Two-eyed Seeing as “walking into two worlds” and recognizing the strengths of both Indigenous and settler knowledge systems (p. 183). Social workers can engage in anti-oppressive and decolonized practice by invoking community members’ ideas for individual healing, as well as program and workshop development, while also resourcing decolonized therapeutic interventions, rather than resorting to mainstream evidence-based practices, which often fail to understand Indigenous ideology and cultural safety.
Anti-Oppressive Practice and Settler-Colonial Education
It is important to examine how our pre-conceived notions or indoctrinations, that are a result of the systems in which we live and work, are maintained by systems of settler colonialism. As a social worker within a colonially dominant culture, I recognize many social workers have been indoctrinated in colonially-developed education systems that tailor intellect in order to fit into mainstream practice (Johnson, 2020; Linklater, 2016). Johnson (2020) states that students (both Indigenous and non-Indigenous) are taught to exclude diverse knowledge systems, such as Indigenous knowledges, and instead are persuaded “to think like a settler” (p. 39). Maracle (1996) states that “the appropriation of knowledge, its distortion and, in some cases, its destruction, was vital to the colonial process” (p. 89). The settler-colonial assimilation process was intended to conform education to the cultural, social and political beliefs of the settler (Thomas & Green, 2020). It was a settler-colonial assumption that Indigenous epistemologies were inferior, which created internalized racism, and supported the settler agenda of domination and colonization (Thomas & Green, 2020).
Thus, we must examine how teachings and training influence our relationships within social work practice. It is important to challenge the settler-colonial paradigms that dominate education, including social work education, which reinforce “altered forms of consciousness” and often separate the head (cognition) and heart (feelings) (Thomas & Green, 2020, p. 43). Settler-colonial education training is often objective, with the direction to assess, recommend, and implement (Thomas & Green, 2020). Many Indigenous traditional paradigms refer to relations and connections with family, community and the land (Gaudet, 2017; Thomas & Green, 2020), as a base for teaching through learning, watching, listening and participating (Stiffarm, 1998). We must examine how we are trained to write case notes and documentation, and we should question whether those case notes are strengths-based and non-pathologizing. Are we acting and writing in a way that best supports the community member? Are we respecting Indigenous traditional teachings within social work practice (Thomas & Green, 2020)? In asking these questions, we can actively evaluate if the social work praxis follows anti-oppressive practice principles.
Anti-Oppressive Practice
The incorporation and implementation of a decolonized, trauma-informed, culturally-safe framework and relationship building is fundamental to anti-oppressive social work practice within Indigenous communities. These frameworks, and how they associate and complement each other, will be discussed more in depth in future sections. In adhering to anti-oppressive practice, certain terms and labels are altered within the body of this chapter, such as replacing the term “client” with “community members,” to diminish the power imbalance and hierarchy that the word “client” may carry. Thomas and Green (2020) state that anti-oppressive practice should include analyzing power differences, examining methods of helping and healing, and exploring who we are and how this practice affects our relationship with people who have been historically and contemporarily marginalized.
A settler-colonial mentality has held the belief that Indigenous peoples and communities need to adapt to settler life and heal and nurture themselves in an evidence-based, specific way. Part of anti-oppressive practice is developing unique plans and programs based on collaboration with the community member and larger community, and utilizing flexibility and creativity rather than prescribing an intervention based solely on clinical perspectives. Clinical perspectives are formed around settler-colonial ideologies and often apply a restrictive biomedical model. As such, it is important to use a client-centered and generalist approach, which recognizes social inequalities while being flexible and versatile in meeting community members’ needs. One way of practicing this may be through developing a holistic healing plan.
A holistic healing plan is flexible, fluid and non-pathologizing. It focuses on the goals of the community member, while also exploring strengths in themselves and their community. A holistic healing plan may include incorporating the medicine wheel to understand how an individual identifies their strengths and areas for improvement mentally, emotionally, physically, and spiritually. However, it should not be assumed that every community uses the medicine wheel. In adhering to an anti-oppressive approach, a holistic healing plan needs to be led by, with, and for the community member, rather than pathologized and clinically created solely by the social worker. A healing plan may also incorporate Indigenous forms of healing and ceremony, although this should not be assumed or enforced based solely on a person’s Indigenous heritage.
Role of Building Relationships
Building relationships within community and with community members, while maintaining relational accountability, is a fundamental element of anti-oppressive practice, and a pillar of culturally-safe, trauma-informed, and decolonized practice. Wilson (2008) describes relational accountability as demonstrating and practicing respect, reciprocity and relationality (The three Rs). Building relationships is essential to establishing trust and respecting boundaries, and is a crucial element of the therapeutic relationship. Creating relationships with community members is a process, and not an inherent right; this must be earned. As previously mentioned, it is important to understand that the process of relationship building with community members can be affected by the trauma inflicted by settler-colonial structures such as health care and social services. Recognizing the historical reasons social workers are viewed as untrustworthy or unsafe is imperative in understanding how current safety is experienced (Greenwood et al., 2017).
When working as an Indigenous or non-Indigenous/settler person within a community that is not your own, it is essential to adapt social work practices by identifying oneself as a guest within the community, and not as an “essential” component. This practice is a part of relationship building, and may include disclosing personal information such as who you are, where you are from, what your cultural background is, how your family relates to Turtle Island, where you went to university/college, and why you are in the community. Sharing and discussing these aspects of self is a way to build relationship and dissolve some characteristics of colonial power dynamics, which can often create a hierarchy of power and control, rather than establishing a trusting, relational practice.
As previously discussed, part of relationship building includes placing oneself as a guest in the community, rather than exercising a role of power and hierarchy, while also sharing personal information in order to create the dynamic of relational social work practice. Community engagement and building relationships might be achieved by honouring/accepting invitations from community members for events, which may coincide with cultural protocol in some communities (Greenwood et al., 2017). Honouring the advice and knowledge of community Elders and knowledge keepers is also imperative in efforts to respectfully engage with community, and coincides with the three Rs by respecting traditional knowledge systems.
Schmidt (2010) notes that it is not uncommon for a rural or remote community to evaluate social workers’ behavior, intentions, personal interests, and groups the social worker is connected with, alongside making inquiries to the social worker that may be considered as “intrusive questions” (p. 12). When we continue to ask community members about their own lives, without disclosing some information about ourselves, it creates a division which is often hierarchical. From a decolonial, culturally-safe perspective, actively participating in relationship building requires relinquishing settler-colonial habits, such as hiding our personal identities as a form of safety, while continuing to analyze community members from a position of power.
Genuine, active listening and engagement are imperative to understanding how individuals envision their healing, through co-creating and recognizing Two-eyed Seeing, rather than imposing colonial therapies and pathologies. A co-creator is a helper who collaborates with community members on their wellness, rather than exclusively deciding and delegating how they should conduct their wellness. Schmidt (2010) recognizes that relationships within rural / small communities are unique because connection and integration with community members is more frequent. Establishing trusting relationships is an important part of forming thoughtful discussions. Genuine and thoughtful discussions are an important part of acting as a co-creator within community engagement, and implementing community members’ ideas for programming, workshops and decolonized therapeutic interventions; social workers should not resort to mainstream evidence-based practices, which often fail to understand Indigenous ideology and cultural safety.
Evidence-based practice in social work has been informed and developed by those with power, as a result of both global and local informational systems of science, positivist and rationalist practice (Beddoe, 2007; 2013). Evidence-based practice thus excludes Indigenous knowledges, and traditional relational approaches to treatment (Beddoe, 2007; 2013). For example, being on the land (in nature), speaking with Elders and knowledge keepers, harvesting and using traditional medicine, and being involved in traditional ceremony enhance physical/biological, mental, emotional and spiritual wellness. These approaches to wellness do not fit the scope of evidence-based practice, and instead settler-colonial therapies and medicines, often developed for and by non-Indigenous people, are recommended. Part of relationship building is to explore what the community member views as healing, which may include the Indigenous methods listed above.
Another aspect of relationship building is understanding role conflict. Schmidt (2010) speaks about the importance of understanding role conflict when building relationships within rural Indigenous communities, as “outsiders coming in” (social workers, non-community members) or “insider[s] coming back” (social workers, who are also community members), and the complexities that they may face (p. 13). Role conflict recognizes the possible difficulties of navigating the lack of anonymity and immersion into the rhythm of community (Schmidt, 2010).
Relationship building is hence a combination of understanding the power dynamics of being a guest in community, building genuine relationships, actively engaging with community, and respectfully understanding community protocol and expectations. Relationship building is imperative in safely and respectfully engaging with community members and with the larger community as a whole.
Cultural Safety
Cultural safety is necessary for practicing anti-oppressive social work within Indigenous communities because of the legacy of colonialism which has created inherent power imbalances. Cultural safety is different than cultural competence. Cultural competence is pan-Indigenous, presuming that all Indigenous nations / communities share the same systems of belief (Yeung, 2016). Cultural safety recognizes the power imbalance between the social worker and the community member, while evaluating the cultural expectations that define treatment and deem which traditions are honoured (Greenwood et al., 2017; Yeung, 2016). Cultural safety is thus a practice of “shifting focus to the experiences of the person receiving care” rather than relying on preconceived ideas or beliefs about a community or nation (Greenwood et al., 2017, p. 182).
Cultural safety prioritizes Indigenous sovereignty and challenges societal hierarchies while necessitating safe practice (Yeung, 2016). Blaikie (2009) states that cultural safety is necessary because of social work codes of ethics and standards of practice which neglect to acknowledge “contextual, cultural and political realities for Indigenous [people]” (p. 3). The characteristics of cultural safety include knowing the history of colonization and its implications within social work practice and society as a whole; adapting social work practice to be community-driven and delegated; following and respecting community protocol while also working with Elders; and working with rather than on Indigenous people, because Indigenous people are experts of their own lives (Kurtz, 2013).
Cultural safety includes adhering to Indigenous knowledge systems and methods of delivering services and understanding Two-eyed Seeing (Greenwood et al., 2017). Two-eyed Seeing dismantles the ideology that healing must be delivered through settler-colonial, evidence-based practices, which ignore and exclude Indigenous knowledge systems as valid, and instead allows the incorporation of both. Crystal Morris, Indigenous traditional medicine practitioner from the Splatsin (Secwepemc) and Tsartlip (WSanec) nations, describes the concept of two-eyed seeing as recognizing the importance of healing methods and herbs that are indigenous to Turtle Island, as well as those that have been introduced through colonialism, in order to support community members and their individualized healing effectively (Morris, 2021).
Two-eyed Seeing creates an ethical space of practice and cultural humility, where Indigenous and non-Indigenous community members and practitioners can establish a safe space for collaboration, creativity and inclusivity—to listen, understand and dream together—in order to move forward (Greenwood et al., 2017). Cultural humility acknowledges that, as practitioners, we commit to a lifelong journey of continued self-evaluation, reflection, and learning, so that we can understand ourselves and our practice (Greenwood et al., 2017). Cultural safety is a way of being both within community practice, and simultaneously in daily individual practices (Kurtz, 2013). Understanding these concepts of cultural safety upholds and respects that healing must be rooted in Indigenous knowledge and values in order to actively support the restoration and reclaiming of these knowledges (Greenwood et al., 2017).
Decolonial Praxis and Connection to Social Work Practice
Colonization is the forced domination and hierarchy that the colonizer creates over the colonized (Kelm, 1998). Social work was developed by settlers and is maintained through settler-colonial structures. Patrick Wolfe (2007) states that “alism is a structure and not an event” (p. 5), highlighting the continuation of colonialism within structures intended for healing, including social work. For this reason, within anti-oppressive practice, social workers must recognize the importance of decolonial praxis. The ambition of absolute decolonization includes prioritizing Indigenous sovereignty, land rights and self-determination (Gahman & Legault, 2017), including the structures intended for health and healing.
Decolonial praxis actively prioritizes Indigenous knowledges, practices, and traditions, and thus works to coincide with cultural safety. The process of decolonization involves challenging settler-colonial policies and systems, so that Indigenous people can “be informed agents of their own lives and healing journey” (Lu & Yuen, 2012, pg. 192). This means to encourage Indigenous sovereignty (decision making) and advocate for Indigenous rights. An example of this may be through challenging systems such as the criminal justice system and adhering to a probation order; for example: advocating for traditional systems of healing (attending a restorative justice healing circle, as a part of a probation order), rather than adhering to settler-colonial law (attending an anger management course as a part of a probation order). Sinclair (2004) affirms that decolonial praxis addresses the historical and current settler-colonial impacts that are maintained through “colonial culture and social suppression, intrusive and controlling legislation, industrial and residential school systems, the child welfare system, and institutional / systemic / individual racism and discrimination” (p. 76).
However, some practitioners, such as Fortier and Wong (2018), state that decolonizing social work is impossible, because the field was developed and is maintained by colonialism. Therefore, Fortier and Wong (2018), call for an unsettling of social work, through:
Deprofessionalization (the restructuring of the ‘helping’ practices of social work back under the control of communities themselves); deinstitutionalization (fighting against the non-profit industrial complex and re-focusing on mutual aid, treaty responsibilities, and settler complicity); and resisting settler extractivism (working towards the repatriation of land, children, and culture and the upholding of Indigenous sovereignty and resurgence). (p. 447)
Part of decolonial social work practice is examining ways in which social work may continue to perpetuate colonial harm. Tuck and Yang (2012) warn against settler harm reduction, which is the act of reducing the harms caused by settler-colonialism, but not seeking to give up privilege, power, and control exercised over Indigenous people and communities (Tuck & Yang, 2012). An example of settler harm reduction would be to focus on a person’s substance use (micro) as the root of their problem, rather than to evaluate the societal and historical impacts (macro) of colonialism, such as lack of housing, land, and resources. As Michelle Alexander (2020), a Black civil rights advocate, states: “we must not be seduced into believing that improving the system is the same as dismantling or transforming it” (p. xxxvii). Practicing this form of settler harm reduction is a method of settler-colonial innocence and continued compliance with the macro structures of colonialism (Tuck & Yang, 2012). Decolonial praxis is thus unsettling social work, rather than attempting to supplement or Indigenize social work (Tuck & Yang, 2012).
Trauma-Informed Practice
The term “trauma” has been created by settlers and has been used to diagnose and pathologize Indigenous experiences of pain and suffering (Linklater, 2016). Furthermore, colonialism is at the root of Indigenous trauma, and this element must be identified in order to take away the blame and shame of trauma from individuals and families (Linklater, 2016). Burstow (2003) describes trauma as “not a disorder but a reaction to a kind of wound” (p. 22). The impact of trauma should be considered interpersonally and intergenerationally, as well as understand the transmission of traumatic experiences and learned behaviours from previous generations. Trauma can affect a person’s (micro) and community’s (mezzo) holistic well-being, emotionally, physically, socially and spiritually, and can be maintained through settler-colonial structures (macro).
For social workers, trauma-informed practice is client-centered and includes being actively aware and conscious about how a community member has been harmed (mentally, emotionally, physically, spiritually) and perceives themselves and their safety in the world. Trauma symptoms, such as “arousal, attention, perception and emotion” can sustain “in altered and exaggerated states long after the specific danger is over” (O’Neill, 2005, p. 75). It is therefore important to acknowledge and recognize that a person’s experience of the present state can be impacted by the trauma they suffered from previously. Trauma-informed practice understands the individual impact of trauma, which is often a result of colonially-created systems (Linklater, 2016), and “strive[s] to provide programs and services which avoid retraumatizing people while supporting their movement towards resilience, recovery and wellness” (Randall & Haskell, 2013, p. 517).
Fortier and Wong (2018) refer to Tuck and Yang (2015) when speaking about how social workers can unintentionally re-traumatize Indigenous people and that we, as social workers, “must recognize settler complicity in colonial violence” (p. 447), which can devalue the experiences of community members. Trauma-informed practice includes culturally-safe practice, recognizing the individual impacts that physical spaces (waiting rooms, offices) can have on a person, and can be perceived as violent or threatening. For example, hospitals and office-settings can resemble that of residential schools, and can cause an inherent visceral trauma reaction (Chansonneuve, 2005). Trauma can also endure through other physical settings such as classrooms, hospitals, and social service offices, which can be seen as unsafe (Brunzell et al., 2016; Perry, 2006). Therefore, being trauma-informed includes being actively engaged in dialogue, identifying the ways in which a person feels safe and in danger, and adapting social work praxis to suit the needs of the community member (client-centered).
Linklater (2016) explains that Indigenous people have experienced increased alienation and trauma when seeking help. It is important to create safe spaces and adjust environments to harmonize with a community member’s needs. An example of adapting spaces to feel safer can include adjusting office space, or practicing social work on the land (land-based). A social worker can engage in a conversation about what setting would make the community member feel more comfortable or safe, such as different lighting, or moving to a different location such as sitting outside. For example, a community member once informed me that the lighting in my office was too dark (it was winter, in the late afternoon and the lights were off in the centre, leaving the room shaded). Although explanations are never needed, the community member explained that they had experienced a traumatic experience in a shaded room. It is important to acknowledge these experiences and adapt the environment to the individual’s need. As previously mentioned, an individual’s or a community’s unique experiences can cause distinct reactions to trauma. Indigenous people and communities have survived settler-colonial attempts to extinguish and assimilate them (Greenwood et al., 2017). Trauma-informed practice recognizes the resilience of community members and communities, as well as unique forms of healing.
Policy and Service Delivery Issues
Settler-colonial policy and service delivery has historically failed to meet the needs of Indigenous individuals and communities. Linklater (2016) explains that these service delivery methods were not created from an Indigenous worldview. The creation of these systems, both within the confines of physical and political boundaries of Indigenous communities, limits relevant services (Pugh & Cheers, 2010; Schmidt, 2010).
Policy and Control
When treaties were first established, Indigenous people believed that their inherent right to traditional Indigenous systems and cultures would be continued and maintained (Robidoux & Mason, 2017). As previously mentioned, current social work practice in Indigenous communities is governed by settler-colonial policy. Although work to “Indigenize” programs and policies are underway—including healing lodges, sentencing circles, restorative justice, treatment centres and health centres—these programs are still maintained and controlled by colonial systems that delegate structure and provide funding, and thus cannot be fully independent (Giannetta, 2021). Giannetta (2021) articulates that the tactic of Indigenizing current colonial systems is a means to maintain power and control, without implementing any meaningful change. An example of this failure to dismantle settler-colonial policy can be seen through examining current healing lodges within the Justice system:
These lodges operate within penitentiaries (a colonial institution) after an Indigenous offender has been sentenced (through a colonial justice system) for committing a crime (defined by the colonial political system) caused by underlining social issues (stemming from colonialism). (Giannetta, 2021, p. 4)
Indigenous communities continue to strive to overcome these barriers through implementing grass roots programs and initiatives. For example, in British Columbia, the First Nations Health Authority (FNHA) is an Indigenous-created and led health authority with the “commitment to engage and privilege Indigenous health and wellness” (Greenwood et al., 2017, p. 185). However, within FNHA programs, barriers of accessibility continue to be prevalent. For example, long wait times for admission to substance use treatment centers, which can be between 1 – 3 months, can be detrimental to healing. Furthermore, similar to non-FNHA treatment centers, many FNHA treatment centers do not support access to harm reduction services and deny the individual’s acceptance to programming if they access Opioid Agonist Therapies (OAT), such as suboxone, methadone or kadian. OAT is a longer-acting opioid that decreases withdrawal and minimizes cravings for individuals who use substances such as heroin, fentanyl and oxycodone. OAT is prescribed by medical professionals. These barriers can lead to sustained or increased use of substances, and overdose.
Delivery of Service
There is undoubtedly a lack of access to social, health and extended services in rural, remote and small Indigenous communities, because of the historical displacement of and disregard for Indigenous people and communities (Pugh & Cheers, 2010; Schmidt, 2010; Zapf, 2010). Some communities have adapted to the lack of services, for example, the First Nations Health Authority (FNHA), discussed in the previous section, has implemented access to virtual doctors, psychiatrists, addictions specialists and counsellors. However, to access these services, individuals need the internet, which is often unavailable in rural and remote areas, including on reservations and in Indigenous communities.
Further injustices leading to barriers are intensified due to resource extraction, and the “rape” of the land (Hunt & Craft, 2021). One example of this is the Dakota Access Pipeline (DAPL), which was originally planned for an area that could potentially affect the water system which serviced non-Indigenous communities (McKibben, 2016). The pipeline was moved to Indigenous land, without the consent of the Standing Rock Indigenous Nation (McKibben, 2016). When Indigenous people and communities voiced their concerns, they were ignored, which led to worldwide attention, and subsequent social justice movements. However, pipelines and resource extraction not only affect the physical health of Indigenous Nations, but they also create worker camps, which directly increase the potential for physical and sexual violence against Indigenous women and girls in surrounding nations, contributing to the epidemic of Missing and Murdered Indigenous Women and Girls (MMIW) (Hunt & Craft, 2021; Macy, 2020).
Barriers to service delivery are exacerbated by a lack of public transportation options, including the cancellation of bus service provided by the Greyhound bus company (Rodriguez, 2021). Access to fewer, or no, options for transportation affects individuals’ ability to access health services and appointments, education, employment and opportunities to meet and gather with family (Rodriguez, 2021). Transportation restrictions have led individuals to choose hitchhiking in order to access these services, which is a safety risk, especially for Indigenous people. The Trail of Tears is one horrific example of Indigenous peoples’ disproportionate risk, referring to a stretch of road where individuals have gone missing or been murdered while hitchhiking; again, increasing the number of Missing and Murdered Indigenous Women and Girls (MMIW) (Levin, 2016).
In order to cope with these barriers, some social work practitioners recommend community-based service delivery, which utilizes Indigenous community strengths, resources and natural helping systems. Zapf (2010) refers to Nelson (1986) when recommending a model of integration of services in various communities in both Canada and Australia. Some of the communities are interagency and include recreation, education, policing and other services that are within, or close to, rural communities (Zapf, 2010). Building on strengths, skills and abilities within the community allows members to access services more quickly.
Community-based service delivery can be enhanced by building capacity within these areas. The purpose of community capacity building is to educate, consult with and train local community helpers so that they can deliver services within that community (Zapf, 2010). Building local expertise and community confidence through natural and informal helping systems is less costly and sustains services in community (Zapf, 2010). Social workers are advised to support natural and informal support systems, and not to replace or supplant (Zapf, 2010). An example of capacity building in addictions services is identifying and supporting a community champion, who may, for instance, identify with having used substances, or is using, and acts as a provider of harm reduction supplies or participates in leading community action teams.
Other barriers to service delivery in community work can include rigid rules and regulations, from “a controlling power of the state” and “conflicting expectations of state, profession, employer, and community” (Zapf, 2010, p. 74). This refers to the power and influence that provincial and federal policy and regulations have on Indigenous communities, and the disregard of Indigenous autonomy. Zapf (2010) encourages social workers to navigate these barriers by dynamically interweaving creative flexibility and collaborating in decision making with the community. Zapf (2010) further explains that social work practice becomes “more intuitive, as the worker comes to rely more on community relationships and less on the authority of knowledge” (p. 75).
Canadian Association of Social Workers (CASW) Code of Ethics
The values present within the CASW (2005) Code of Ethics that are distinct when working with rural / small Indigenous Communities include advocating for equitable services and challenging injustices [Value 2], which, as previously mentioned, are barriers when working within these communities. The CASW (2005) Code of Ethics states that social workers must understand the power imbalance that occurs in a social work-community member relationship, while prioritizing the needs of the individual [Value 3]. Value 3 (CASW, 2005) also states that a social worker should use their professional knowledge and skills when working with a community member. However, social workers must acknowledge the history of settler colonialism and engage in collaborating and implementing Indigenous knowledge systems and healing, as these pertain to the community/community member.
Registered social workers are accountable to the Canadian Association of Social Workers (CASW, 2005), and the provincial/territorial associations and colleges, and are required to adhere to a standard of practice, ethics and values. An important focus in the CASW (2005) Code of Ethics, and stressed by Arges et. al. (2010), is that social workers have an obligation to uphold:
The welfare and self-realization of all people; the development and disciplined use of scientific and professional knowledge; the development of resources and skills to meet individual, group, national and international changing needs and aspirations; and the achievement of social justice for all. The profession has a particular interest in the needs and empowerment of people who are vulnerable, oppressed, and/or living in poverty. (CASW, 2005, p. 3)
This statement is not particularly anti-oppressive in its wording, since it suggests that social workers can label and define who is considered vulnerable or oppressed, alongside highlighting the use of scientific and professional knowledge, rather than community and traditional knowledge. However, it nonetheless stresses the importance of upholding individual and community needs, and of social justice. This would suggest that the role of social workers is to work with, rather than on, community members.
The TRC and UNDRIP
The CASW (2005) Code of Ethics also mentions the importance of honoring the Canadian Charter of Rights and Freedoms (1982) and the United Nations Universal Declaration of Human Rights (1948). Other relevant reports pertaining to Indigenous people, made by and for Indigenous people, include Truth and Reconciliation Commission of Canada: Calls to Action (TRC, 2015) and the United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP, 2008).
The TRC (2015) has created calls to action that specifically name and call upon social workers to be educated and trained when working with Indigenous communities, so that they will provide culturally-safe and “appropriate solutions to family healing” (p. 1). Other areas recognized in the TRC (2015) are the call for recognizing and valuing community-controlled Indigenous healing practices and working with Indigenous healers and Elders. Giannetta (2021) reflects on these elements when stating that systems of healing and being must be implemented, and not expected to “operate within the confines and to the discretion of” settler-colonial systems (p. 7).
Social workers should be educated about the implementation of UNDRIP and honour / abide by the Indigenous collective rights therein (Greenwood et al., 2017). UNDRIP (2008) calls for the restoration, reclamation and sharing of Indigenous knowledge of health, while also acknowledging the settler-colonial influences in “harmful systems, organizations and relationships” that perpetuate harm (Greenwood et al., 2017, p. 182). Indigenous knowledge is “embedded in Indigenous languages, cultures, lands and territories, and laws and ceremonies” and must be implemented, in a culturally-safe way, into social work practice (Greenwood et al., 2017, p. 182).
The UNDRIP (2008) document calls upon settler-colonial policies and practices that disregard Indigenous practices as invalid to be abolished. UNDRIP (2008) states that Indigenous people have the right to exercise their rights, which include having autonomy in individual and community decision making, and maintaining and practicing holistic (mental, emotional, physical, spiritual) health practices, including traditional medicine and ceremony; it also stresses the right to live on their traditional territories and access resources, preventing further dispossession. UNDRIP (2008) identifies the boundaries that Canada and the Canadian government is required to adhere to, including working harmoniously with Indigenous people by recognizing and granting Indigenous sovereignty and rights, and by also dismantling and deconstructing any forms of assimilation or destruction of culture. UNDRIP (2008) further indicates that the State must allow for Indigenous nations to maintain and/or re-develop Indigenous institutions for decision making.
Conclusion
Audre Lorde’s famous essay articulates, “the master’s tools will never dismantle the master’s house” (1984). The tools of settler-colonialism have created a system of social services and social work that has not developed to maintain the wellness of Indigenous communities. The core of anti-oppressive practice is to actively engage in decolonization and advocating for autonomy for Indigenous people and communities, while practicing social work with a culturally-safe and trauma-informed lens. It is through these relationships and practices that social workers can create a new narrative as active co-creators and healers within Indigenous communities, rather than continuing to practice as settler-colonial saviours.
Activities and Assignments
- Personal Research: Understand yourself/family/community history on Turtle Island.
- Did your family immigrate to Turtle Island, and (if so) when and from where?
- What cultures / languages did your ancestors practice / speak? Do you practice / speak these cultures and languages?
- Has colonialism / settler colonialism affected you or your ancestors, and how?
- Community relationships:
- In evaluating the chapter contents, which ways might dominant social work differ from community social work in Indigenous communities?
- CASE STUDY: Imagine you are a new social worker within an Indigenous community. A community Elder visits you at the office and begins to ask you questions about your reason for being in community. How can you respond in an anti-oppressive, culturally- safe, trauma-informed way?
- CASE STUDY: A community member, with whom you have worked with throughout their healing journey and goal of sobriety, “graduates” from their substance-use treatment program. At the ceremony, the community member gifts you with a craft they had made. How do you navigate community protocol and the ethics of the CASW?
Additional Resources
- Linklater, R. (2016). Decolonizing trauma work: Indigenous stories and strategies. Langara College.
- Tuck, E., & Yang, K. W. (2012). Decolonization is not a metaphor. Decolonization: Indigeneity, Education & Society, 1(1), 1-40.
- Fortier, C., & Wong, E. H. (2018). The settler colonialism of social work and the social work of settler colonialism. Settler Colonial Studies, 9(4), 437-456.
- Truth and Reconciliation Commission of Canada. (2015). Truth and reconciliation commission of Canada: Calls to action. http://www.trc.ca/assets/pdf/Calls_to_Action_English2.pdf
- United Nations Declaration on the Rights of Indigenous Peoples. (2008). United Nations. https://www.un.org/esa/socdev/unpfii/documents/DRIPS_en.pdf
References
Aboriginal Healing Foundation. (2006). Métis History and experienced and Residential Schools in Canada. https://www.ahf.ca/downloads/metiseweb.pdf
Alexander, M. (2020). The new Jim Crow: Mass incarceration in the age of colorblindness (10th ed.). The New Press.
Arges, S., Abdulahad, R., & Delaney, R. (2010). Deconstructing the southern metaphor: Moving from oppression to empowerment. In R. Delaney and K. Brownlee (Eds.), Northern & Rural Social Work Practice: A Canadian Perspective (pp. 18-42). Hignell Book Printing.
Australian Human Rights Commission. (2001, December 2). Bringing them home – Frequently asked questions about the National Inquiry. www.humanrights.gov.au/social_justice/bth_report/about/faqs.html#ques9
Bateman, R. (1996). Talking with the plow: Agricultural policy and Indian farming in the Canadian and U.S. Prairies. The Canadian Journal of Native Studies XVI(2), 211-228. http://www3.brandonu.ca/cjns/16.2/bateman.pdf
Bear, C. (Host). (2008, May 12). American Indian Boarding Schools Haunt Many. In Morning Edition. NPR. https://www.npr.org/templates/story/story.php?storyId=16516865?storyId =16516865
Beddoe, L. (2007). Change, complexity, and challenge in social work education in Aotearoa, New Zealand. Australian Social Work, 60(1), 46-55.
Beddoe, L. (2013). ‘A profession of faith’ or a profession: Social work, knowledge and professional capital. New Zealand Sociology 28(2), 44-63.
Bleau, D., & Dhanoa, J. (2021). Behind the front lines: Realities of racism and discrimination for IBPOC social workers [Manuscript submitted for publication].
Brunzell, T., Stokes, H., & Waters, L. (2016). Trauma-informed flexible learning: Classrooms that strengthen regulatory abilities. International Journal of Child, Youth & Family Studies, 7(2), pp. 218-239.
Canadian Association of Social Workers. (2005). CASW code of ethics. https://www.casw-acts.ca/files/documents/casw_code_of_ethics.pdf
Chansonneuve, D. (2006). Reclaiming connections: Understanding residential school trauma among Aboriginal people. Aboriginal Healing Foundation.
Collier, K. (1984). Social work with rural peoples. New Star Books.
Collier, K. (1993). Social work with rural peoples (2nd ed.) New Star Books.
Collier, K. (2006). Social work with rural peoples (3rd ed.). New Star Books.
Delaney, R. (2009). The philosophical and value base of Canadian social welfare. In F. Turner & J. Turner (Eds.), Canadian social welfare (6th ed., pp. 8-23). Prentice Hall, Allyn and Bacon.
Fortier, C., & Wong, E. H. (2018). The settler colonialism of social work and the social work of settler colonialism. Settler Colonial Studies, 9(4), 437-456.
Gahman, L., & Legault, G. (2017). Disrupting the settler colonial university: Decolonial praxis and place-based education in the Okanagan Valley (British Columbia). Capitalism Nature Socialism, 30(1), 50-69.
Gaudet, C. (2017). Pimatisiwin: Women, wellness and land-based practices for Omushkego youth. In M. A. Robidoux & C. W. Mason (Eds.), A land not forgotten: Indigenous food security & land-based practices in Northern Ontario. University of Manitoba Press.
Giannetta, R. (2021). Canadian justice/Indigenous (in)justice: Examining decolonization and the Canadian criminal justice system. Journal for Social Thought 5(1), 1-11.
Greenwood, M., Lindsay, N., King, J., & Loewen, D. (2017). Ethical spaces and places: Indigenous cultural safety in British Columbia health care. Alter Native: An International Journal of Indigenous Peoples, 13(3), 179-189.
Hart, M., Sinclair, R., & Bruyere, G. (2010). Wícihitowin: Aboriginal social work in Canada. Langara College.
Hunt, S. & Craft, A. (2021, February 26). Sovereignty, intimacy, and resistance: Legal and relational responses to gendered violence and settler colonialism [Webinar]. University of Guelph.
Jacobs, M. C. (2012). Assimilation through incarceration: The geographic imposition of Canadian law over Indigenous people [Unpublished doctoral dissertation]. Queen’s University.
Johnson, H. (2020). Peace and good order: The case for Indigenous justice in Canada. CNIB.
Joseph, B. (2018, November 27). Insight about 10 myths about Indigenous peoples. Indigenous Corporate Training.
Kamin, A., & Beatch, R. (1999). A community development approach to mental health services. In R. Delaney, K. Brownlee, & M. Sellick (Eds.), Social work with rural and northern communities (pp. 303-315). Lakehead University Centre for Northern Studies.
Kelm, M. E. (1998). Colonizing bodies: Aboriginal health and healing in British Columbia, 1900-50. UBC Press.
Kestler-D’Amours, J. & O’Toole, M. (2019, December 5). Nations divided: Mapping Canada’s pipeline battle. Pulitzer Centre.
Kurtz, D. L. (2013). Indigenous methodologies: Traversing Indigenous and Western worldviews in research. AlterNative: An International Journal of Indigenous Peoples, 9(3), 217-229.
Levin, D. (2016, May 24). Dozens of women vanish on Canada’s highway of tears, and most cases are unsolved. The New York Times.
Linklater, R. (2016). Decolonizing trauma work: Indigenous stories and strategies. Langara College.
Locke, B. L. & Winship, J. (2005). Social work in rural America: Lessons from the past and trends for the future. In N. Lohmann and R.A. Lohmann (Eds.), Rural social work practice (pp. 1-24). Columbia University Press.
Lorde, A. (1984). The master’s tools will never dismantle the master’s house. Sister Outsider: Essay and Speeches (pp. 110-114). Crossing Press.
Lu, L., & Yuen, F. (2012). Journey women: Art therapy in a decolonization framework of practice. Elsevier Journal: The Arts In Psychotherapy, 39, 192-200.
Macy, E. (2020). Don’t bite the hand that feeds you: Environmental and human exploitation sold as prosperity. Tapestries: Interwoven voices of local and global identities, 9(1), Article 4.
Maracle, L. (1996). I am woman: A Native perspective on sociology and feminism. Press Gang Publishers.
Martinez-Brawley, E. (2000). Close to home: Human services and the small community. NASW Press.
McKibben, B. (2016, September 6). A pipeline fight and America’s dark past. The New Yorker.
Morris, C. (2021, April 8). Sharing Mela’hma. [Presentation]. Aboriginal Mental Wellness – Community of Practice, BC, Canada.
Nelson, C.H. (1986). Innovations in northern/rural community-based human service delivery. [Paper presentation]. Learned Societies Conference, Winnipeg, MB, Canada.
O’Neill, E. (2006). Holding flames: Women illuminating knowledge of s/Self transformation [Unpublished doctoral dissertation]. University of Toronto.
Official Report of the Nineteenth Annual Conference of Charities and Correction. (1892). In R. H. Pratt (Ed.), The advantages of mingling Indians with whites (260–271). Harvard University Press.
Perry, B. (2006). Fear and learning: Trauma-related factors in the adult education process. New Directions for Adult and Continuing Education, 110, 21-27.
Pratt, R. H. (1892, June 23-29). The advantages of mingling Indians with Whites. In Isabel C. Barrows (Eds.). Proceedings of the National Conference of Charities and Correction (pp. 45-59). Geo. H. Ellis Press.
Pugh, R., & Cheers, B. (2010). Rural social work: An international perspective. Policy Press.
Robidoux, M. A., & Mason, C. W. (2017). A land not forgotten: Indigenous food security & land-based practices in Northern Ontario. University of Manitoba Press.
Rodriguez, J. (2021, May 25). Indigenous, rural residents left ‘more isolated’ after Greyhound leaves Canada. CTV News. https://www.ctvnews.ca/canada/indigenous-rural-residents-left-more-isolated-after-greyhound-leaves-canada-1.5442354
Schmidt, G. (2010). What is northern social work?. In R. Delaney and K. Brownlee (Eds.), Northern & rural social work practice: A Canadian perspective (pp. 1-17). Hignell Book Printing.
Shepherd, R., & McCurry, P. (2018, October 31). Ottawa must talk to Canadians about nation-to-nation agenda. Policy Options.
Sinclair, R. (2004). Aboriginal social work education in Canada: Decolonizing pedagogy for the seventh generation. In First Peoples Child & Family Review, 1(2), 49-61.
Statistics Canada (2018). Rural area (RA). https://www150.statcan.gc.ca/n1/pub/92-195-x/2011001/geo/ra-rr/ra-rr-eng.htm
Stiffarm, L. A. (1998). As we see–: Aboriginal pedagogy. University Extension Press.
Thomas, R., & Green, J. (2020). A way of life: Indigenous perspectives on anti-oppressive living. First Peoples Child & Family Review, 3(1), 91-104.
Truth and Reconciliation Commission of Canada. (2015). Truth and reconciliation commission of Canada: Calls to action. http://www.trc.ca/assets/pdf/Calls_to_Action_English2.pdf
Tuck, E., & Yang, K. W. (2012). Decolonization is not a metaphor. Decolonization: Indigeneity, Education & Society, 1(1), 1-40.
Tuck, E., & Yang, K. W. (2014). Unbecoming claims. Qualitative Inquiry, 20(6), 811-818.
United Nations Declaration on the Rights of Indigenous Peoples. (2008). United Nations. https://www.un.org/esa/socdev/unpfii/documents/DRIPS_en.pdf
van der Kolk, B. (2015). The body keeps the score: Brain, mind, and body in the healing of trauma. Penguin Books.
Walker, C. (2015, May 29). New documents may shed light on residential school deaths. CBC News. https://www.cbc.ca/news/indigenous/new-documents-may-shed-light-on-residential-school-deaths-1.2487015
Wilson, S. (2008). Research is ceremony: Indigenous research methods. Fernwood Pub.
Wolfe, P. (2007). Settler colonialism and the elimination of the native. Journal of Genocide Research, 8(4), 387-409.
Yeung, S. (2016). Conceptualizing cultural safety: Definitions and applications of safety in health care for Indigenous mothers in Canada. Journal for Social Thought, 1, 1-13.
Zapf, M. K. (1985). Rural social work and its application to the Canadian north as a practice setting (Vol. 15, Working Papers on Social Welfare in Canada). University of Toronto.
Zapf, M. K. (2010). Northern service delivery: Strategies and considerations. In R. Delaney and K. Brownlee (eds.), Northern & rural social work practice: A Canadian perspective (pp. 1-17). Hignell Book Printing.
In line with a feministic perspective the authors would like to recognize that there is no hierarchy in the contributive efforts of this chapter and acknowledge that this chapter would not have been possible without the differing intersectional perspectives of each author.
Violence against women is still prevalent in Canadian society and directly impacts not only women and their families, but also the collective community. In rural, remote, and northern communities across Canada, pre-existing vulnerabilities and risk of violence against women[1] is increased and often experienced through Intimate Partner Violence (IPV) and Domestic Violence (DV). The frequency of violence against women is a direct reflection of the ongoing social problems in Canada resulting in the inequality of women (e.g., historical, social, political, cultural, and economic, etc.). Conroy (2021) identifies that in 2019, the rates of family violence in remote and rural Canadian communities was 2.0 times higher than in the rest of Canada, and intimate partner violence was 1.8 times higher in rural and remote communities.
While these statistics are concerning, Gracia (2004) suggests that the majority of IPV and DV against women often goes unreported due to a multiplicity of societal oppression(s), personal circumstances, and barriers to accessing support. However, those who live with multiple intersectional ties may be at a higher risk of violence, particularly Indigenous, immigrant, and Lesbian/Bisexual/Transgender/Intersex (LBTI) women living in rural, remote, and northern regions (Calton et al., 2016; Daoud et al., 2013; Murshid & Bowen, 2018).
This chapter focuses on IPV against women in rural, remote, and northern regions. However, it should be noted that while women may also perpetuate violence, that will not be the focus of this chapter. Furthermore, it provides an opportunity to learn and reflect on the prevalence of IPV and DV in rural, remote, and northern communities within Canada and how social work practitioners support the work being done at the micro, mezzo, and macro levels. Social workers providing services in these communities need to be aware of risks, how to provide risk assessment, and how to incorporate safety considerations for those who may be experiencing IPV and DV.
[1] In this chapter the term “woman/women” refers to cisgender, trans, intersex, and anyone identifying as a “woman.”
Learning Objectives
By the end of this chapter, the following learning objectives should be achieved:
- Understanding of definitions of IPV and DV and awareness of the rates and the historical context for this issue in Canada, specifically in rural, remote and northern communities
- Awareness of implications for social workers working with victims of IPV and DV in rural, remote, and northern communities across Canada
- Understanding of specific safety planning and practice considerations for social work professionals on a micro, mezzo, and macro level
- Awareness of the importance for social workers to develop collaborative working relationships, and educational and advocacy opportunities to reduce the severity and frequency of IPV and DV occurrences.
Theoretical Framework
The complexity of violence and its impact may be best understood through a feminist, trauma-informed, intersectional lens. In alignment with a feminist perspective, this chapter uses the term “survivor,” rather than “victim,” as the word “victim” pathologizes and disempowers the woman who has experienced violence (Walker, 2002). Feminist theology serves to empower women and raise awareness that disparity and oppression within larger, structural, and political systems exist (Corbeil et al., 1983, as cited in Walker, 2002). In combination with a trauma-informed lens, principles grounding our understanding of domestic violence include the following: safety, trustworthiness and transparency, collaboration and peer support, empowerment, and choice for survivors (Bowen & Murshid, 2016). Applying these principles in understanding violence, in order to support survivors, highlights a useful approach to providing care that is not re-traumatizing. In addition, using an intersectional lens allows individuals to gain a deeper understanding of IPV and DV. For example, Sokoloff and Dupont (2005) explain that violence experienced and reflected among an individual’s social locators (e.g., culture) may be interpreted by the survivor differently than by witnesses or observers. Therefore, it is important to be aware that cultural differences should not mask the larger systemic and structural forms of oppression (e.g. racism, colonialism, sexism, heterosexism, ableism, patriarchy, economic exploitation, etc.) that impact and increase violence for women across diverse social locators (Sokoloff & Dupont, 2005).
History of Domestic Violence in Rural, Remote and Northern Communities
Canada is a vast country, with most of its population residing in large urban cities (Moffitt et al., 2020) and an estimated 19% of Canadians in rural and remote areas (Statistics Canada, as cited in Graham et al., 2017). Historically, the violence perpetrated against women has been embedded in many institutions and remains entrenched covertly and overtly in our current systems. For example, the women’s suffrage movement and resistance against the dominant, patriarchal Canadian society began in Manitoba in 1916 (Parliament of Canada, n.d.). Other provinces, such as Saskatchewan and Alberta, followed suit until, on a federal platform, Canada conceded to the pressures of change (Parliament of Canada, n.d.). However, while there were a number of significant changes and rights acknowledged in the 20th century, violence against women continues to be a significant issue (Sitter, 2017). Walker (2002) highlights that during the 1970s, a network of shelters was developed across North America in response to violence against women (Government of Canada, 2021b).
Service Delivery
The delivery of safety services for survivors of IPV continues to be an area of advocacy research/development and ongoing evaluation for social workers in Canada. While DV does not differentiate among geographical locations, social workers working in rural, remote and northern areas of Canada have unique service delivery needs and limitations based on resources and location. The implementation of IPV policies that have been developed and implemented in more densely populated areas of Canada are often inadequate in meeting the needs of rural, remote, and northern communities.
Policy
Policy development for IPV and DV continues to be an area of concern, since several Canadian provinces lack legislation to support the survivors of violence. In 2021, six provinces (Alberta, Manitoba, Newfoundland and Labrador, Nova Scotia, Prince Edward Island and Saskatchewan) and three territories had implemented legislation to support survivors of IPV, in addition to the laws set forth in the Canadian Criminal Code (Government of Canada, 2021b). The Criminal Code is meant to prohibit some forms of IPV, including “physical and sexual assault, some forms of emotional/psychological abuse and neglect, and financial abuse” (Government of Canada, 2021a, para. 3); however, further support is required to address intimate partner violence (IPV) across Canada.
As part of the Canadian Advisory Council on the Status of Women’s work conducted in 1980, there were key changes and suggestions made and implemented in the Criminal Code to address the issue of IP V at the time (Ad Hoc Federal-Provincial-Territorial Working Group, 2017). Other examples include an amendment in 1983 to protect partners in their intimate relationships from such acts as spousal rape, and in 1993 to include criminal harassment (i.e., stalking) (Government of Canada, 2021b). More recently,
…in June 2019, the Criminal Code was amended to strengthen the criminal justice’s response to IPV, including by defining ‘intimate partner’ for all Criminal Code purposes and clarifying that the term includes a current or former spouse, common-law partner and dating partner. (Government of Canada, 2021b, para. 5)
With that said, between 1974 and 2001, there was a 62% decrease of spousal homicides, suggesting that many of the changes had the desired effect (Ad Hoc Federal-Provincial-Territorial Working Group, 2017).
Provincial policymakers have continued to address the issue of IPV in provinces, such as in Saskatchewan where rates are above the national average, by developing legislation such as the Interpersonal Violence Disclosure Protocol “Clare’s Law” (Government of Saskatchewan, 2021). First implemented in Britain in 2014, Clare’s Law has been adopted, not only by the vast majority of municipal police in cities across Saskatchewan, but also more recently by the RCMP (Canadian Domestic Homicide Prevention Initiative, 2021; Government of Saskatchewan, 2021). With Clare’s Law, an applicant can make a request regarding access to information about an individual’s history and past criminal charges which may be disclosed by the proper authorities if they believe that the person they are disclosing to is currently at risk (Canadian Domestic Homicide Prevention Initiative, 2021). These policy changes provide increased safety options for survivors of violence and promote choice and empowerment for survivors in collaboration with social workers and RCMP/police professionals.
The Impact of Domestic Violence
Not only is IPV and DV devastating for the survivor of the relationship, but its implications are also far reaching and may affect the entire family, particularly if children and/or adolescents are living in the family home. IPV also has impact on communities (large and small) and can be particularly devastating when combined with factors that further enhance the vulnerability of individuals and communities.
Childhood & Adolescence
As researchers, organizations and frontline staff who work with women and children who experience IPV and DV, there is an emphasis on interventions and prevention strategies. Cervantes and Sherman (2021) state that early exposure to violence in the home increases the chances that the cycle of violence will continue later in life for those children. Repeated witnessing of these behaviours normalizes this interaction, and children further learn this behaviour by imitating what they observe (Bandura, 1997). Therefore, exposure to violence in the home may increase a child’s risk of expecting, engaging in, and tolerating violent behaviour in their own intimate relationships, thus continuing the cycle of violence intergenerationally (Cervantes & Sherman, 2021). The schemas developed by children and adolescents in terms of intimate relationships are often replicated, unless an individual is exposed to a new environment, which can then become a catalyst for change (Cervantes & Sherman, 2021). Martz et al. (2016) note that their research demonstrated that rural adolescents were at an increased risk for physical and sexual violence with their intimate partners, when compared to urban adolescents. This research is troubling as rural adolescents, and adults, have even less access to information, social supports, and formal services in their communities.
First Nations, Metis & Inuit Women
Colonialism has damaged and changed traditional cultural beliefs in First Nation, Metis and Inuit communities towards women. Daoud et al. (2013) note that before colonialism, women in these cultural communities held respected and valued roles, and it was unthinkable to engage in violence against women. Conroy (2021) identifies that due to historical and ongoing colonialism in Canada, IPV is a direct result of compounding factors such as residential schools, the 60s Scoop, the child welfare system, and murdered and missing Indigenous women. These factors can combine in creating intergenerational trauma, addiction, and poverty, as well as enforcing traditional, euro-centric, christian gender roles on Indigenous women (Daoud et al., 2013). Studies demonstrate that rates of violence are considerably higher among Indigenous women, especially in rural and remote areas in Canada (Brownridge, 2008) where Indigenous women experience IPV eight times more than non-Indigenous women (Daoud et al., 2013). In consideration of these disturbing statistics, Moreau (2019) notes that in 2017/2018 there were 522 domestic violence shelters across Canada, and only 30 of these shelters located on reserves. Daoud et al. (2013) argues that due to colonization, violence was introduced and still impacts the community in multiple ways. The first is through collective violence in the form of institutional discrimination that attacks human rights for Indigenous communities. The next is forcing patriarchal and Christian values onto Indigenous communities resulting in a shift in their gender roles and the balance of power among genders. The third distinction is a result of colonial policies, such as residential schools. Intergenerational trauma was perpetrated with the removal of children from their families, communities and culture, and the experience of abuse (physical/emotional/sexual/cultural) while in care. Intergenerational trauma from childhood experiences often results in family and intimate partner violence later in children’s lives.
The violence continues to be so pervasive that campaigns, such as Amnesty International’s Stolen Sisters, have been initiated to increase awareness around the higher rates of violence and discrimination perpetrated against First Nations women (Amnesty International, 2004). Statistics suggest that this group is six times more likely to be killed (Howard, 2021), and Oppal (2012) reported that First Nations, Metis, and Inuit women represent 10% of all female homicides, which is significantly disproportionate compared to the overall national crime rate against women.
Indigenous women living in remote, rural, and northern communities in Canada can also face significant barriers to leaving an abusive relationship, such as not wanting to leave one’s family community or reserve (Campbell et al., 2003), limited or no access to a shelter, lack of support, and the cost of travel. These compounding challenges, combined with intergenerational trauma, contributes to ongoing colonialism in First Nations communities. Elders tell stories of the impact of colonization, the introduction of alcohol and disease, and the mistreatment of women (Moffitt et al., 2020). According to the World Health Organization (WHO), alcohol consumption can further increase the risk for IPV. For example, excessive use of alcohol was identified as a risk factor for intimate partner homicide in 40% of cases reviewed in Ontario between 2003 and 2017 (Office of the Chief Coroner Province of Ontario, 2018).
Newcomers to Canada
Another vulnerable population to consider in rural, remote, and northern locations is newcomers to Canada. These women face further unique barriers when living in these regions, such as discrimination (e.g. racism), culture shock, communication (e.g. language) and immigration status (Ford-Gilboe et al., 2015; Murshid & Bowen, 2018; Sandberg, 2013; Sokoloff & Dupont, 2005). While many immigrant and refugee women experience barriers, these women are often dependent on their partners who perpetuate the abuse (Sandberg, 2013). This dependency may include financial dependency (education in other countries may not transfer), isolation from the cultural community, understanding IPV laws in Canada (Murshid & Bowen, 2018), lack of awareness of services (Ford-Gilboe et al., 2015), and the inability to leave the current home (Sandberg, 2013). The individuals perpetrating violence gain power and control by exploiting threats of deportation, reinforcement of patriarchal gender roles and relationships, and fear of losing custody of their children (Murshid & Bowen, 2018). Leaving the relationship is difficult due to discrimination experienced from a variety of sources including consideration of housing options and police involvement (Murshid & Bowen, 2018). Police may be under-educated or hold immigration bias/racist beliefs and may view the violence as a cultural attribute (Sokoloff & Dupont, 2005).
Lesbian, Bisexual, Transgender, and Intersex (LBTI) Women
One major unique barrier facing women in the Lesbian, Bisexual, Trans and Intersex (LBTI) community is a lack of knowledge and information possessed by service providers regarding LBTI issues and various forms of discrimination connected with this intersectionality. Kay and Jefferies (2010) explain that due to our heteronormative society, the classical definition and understanding of IPV is that a woman is harmed by a male. Furthermore, the two spirited, lesbian, gay, bi-sexual, transgender, queer, intersex and a-sexual plus (2SLGBTQIA+) community education around IPV is insufficient and 2SLGBTQIA+ individuals experiencing IPV may not classify their experiences as violence due to dominant cultural templates (Calton et al., 2016). Further, education in this area for professionals is severely lacking. Survivors seeking help may encounter further discrimination and stigma by law enforcement, the court system, and by helping professionals (e.g. homo/bi/transphobia), which may result in returning to their abuser and/or not reporting or seeking help for future occurrences (Calton et al., 2016; Sokoloff & Dupont, 2005). Renzetti (1998) notes the complexity that internalized homophobia plays as a contributing factor, as the survivor fears disclosing the violence. LBTI perpetrators of violence use internalized homophobia and the fear of discrimination by service providers and the community to gain more power and control over their partners (Sokoloff & Dupont, 2005). They often use the tactic of threatening to “out” their partner (Sokoloff & Dupont, 2005), and emphasize the potential risk of losing one’s children, employment, relationships (family/friends/community) or housing (Calton et al., 2016). Peterman and Dixon (2003) identified that if shelters are available for LBTI users, there is a unique risk that the perpetrator may enter the “safe” space (i.e. shelter) and commit further abuse and/or harass their partner. As well, service providers or residents at these shelters may be homo/bi/transphobic making them unsafe (Sokoloff & Dupont, 2005).
Barriers to Service Delivery
Due to the complexity and multilevel experiences of oppression, Murray et al. (2015) note that women often do not make an immediate decision to leave a violent partner/situation after a single incident; it is usually after gradual increases in violence that survivors make this decision. Furthermore, survivors of intimate partner violence and domestic violence will often leave and later return to their partner who perpetrated abuse multiple times before leaving for good (Murray et al., 2015). To begin understanding the barriers that face women living in rural, remote, and northern geographies experiencing IPV and DV, we suggest that social workers reflect on the four levels of oppression that are involved: societal/cultural, institutional, interpersonal, and personal.
Societal and Cultural
Sexism, patriarchy, Catholicism, racism and traditional “family values” still affect the lives of Canadian women. These oppressive ideologies often are more prominent and reinforced in rural communities. Wendt and Hornosty (2010) state that patriarchal attitudes, gender stereotypes, traditional family units, and traditional gender roles are interwoven with rural values. These large oppressive structures and ideologies trickle down and reinforce violence against women which can make it difficult for them to leave abusive situations in rural, remote, and northern communities.
The impact of COVID-19 on IPV and DV situations has also added an additional layer of complexity for women. Women who were experiencing IPV/DV before and into the pandemic were further isolated from opportunities/resources as health orders for public safety iterated stay home orders and physical distancing. Fears of exposure to the virus, not being able to access shelters, and feeling the need to stay home with their partners prevented many survivors from reaching out during this time (Moffitt et al., 2020). Survivors who were already isolated due to geographical location had a decrease in chances that a neighbour might potentially overhear/witness or intervene during a violent episode (Sandberg, 2013), and a new barrier was thus created by the virus with the narrative that isolation equals safety (Moffitt et al., 2020). In addition, the impact of the pandemic with factors of higher stress levels on individuals and families (e.g., partners losing work, children’s remote learning) led to increased risk for controlling behaviors and/or heightened barriers for accessing support (Moffitt et al., 2020).
Institutional
Women living in rural, remote, and northern communities face further oppression as the societal beliefs recur within institutions, and survivors encounter unique barriers due to the geographical location they reside in. Research shows that many rural communities pride themselves on “moral lifestyles,” including the sanctity of marriage, family life, and Christian- centered values that serve as the foundation of their town. For example, the institution of marriage impacts survivors of IPV and DV; Cervantes and Sherman (2021) conclude that many women believe that the abuse they encounter is a consequence of marriage. This patriarchal belief instills in women the conviction that, due to their decision to marry (“for better or for worse”), they must endure the abuse no matter how violent the experience. Furthermore, Wendt and Hornosty (2010) comment that in rural life, masculine power and privilege is publicly visible. This privilege is often seen in farming organizations, bars, municipal governments, and sports teams. In terms of local municipal government, Edwards (2015) comments that in certain rural, remote and northern communities, individuals in power may hold the belief that IPV is non-existent and therefore less government involvement in providing preventative or crisis services is needed.
Women experiencing IPV and DV living in rural, remote, and northern locations face increased difficulty accessing services than their urban counterparts. These services may include daycare, community resources, law enforcement (Edwards, 2015), transportation, social services, courts, and shelters (Sandberg, 2013). Services are frequently lacking and limited due to lower population density than is needed to create or receive funding (Phillips & McLeroy, 2004), and the information regarding services is not easily accessible. If services are available, barriers may include issues related to privacy and anonymity, poverty (Edwards, 2015), lack of response from service providers due to long waitlists, being placed on a waitlist, difficulty getting information (Ford-Gilboe et al., 2015), and geographical isolation from community and social support (Sandberg, 2013). Sandberg (2013) notes that the often-low socioeconomic reality of isolated communities results in lack of infrastructure, poor road conditions, lack of job opportunities, and fewer voluntary supports. Regarding law enforcement, Websdale and Johnson (1997) found that rural law enforcement had longer wait times when called and individuals were lucky if police even showed up regarding DV situations. This delay in time-sensitive support and medical care in rural, remote, and northern communities results in increased risk of homicide, due the severity of the inflicted injuries (Gallup-Black, 2005). Additionally, specialized services ranging from police, lawyers, social supports, local courts, and judges often lacked specialized training in IPV and DV (Sandberg, 2013).
Interpersonal
Cervantes and Sherman (2021) identify that, within rural, remote and northern contexts, a commonly-held belief is that domestic violence is not a community problem/responsibility but a personal issue that should remain private. Cohen and Nisbetter (1994) emphasize that rural communities pride themselves on a “culture of honor” which stays quiet and accepts violence, especially if it puts a family’s reputation at risk. This self-preservation at the community level, with the additional barriers of geographic location, makes it difficult for women to find support or resources. Dekeseredy and Schwartz (2009) identify that a safety risk more specific to rural communities occurs when the individual who perpetuates violence has high social capital and, as a result, the likelihood of the tight-knit community supporting the woman is low. Regarding safety, Sandberg (2013) comments that in rural life, conflicts of interest and anonymity are almost non-existent. Law enforcement, social workers, and medical professionals are likely to have a personal relationship with the individual who perpetuates abuse, and safe houses may be difficult to keep invisible from that individual.
Personal
Identity for rural women becomes a potential barrier to services, as Wendt and Hornosty (2010) state that many rural women who have a strong identity with the land, community, and preservation of the family may stay in abusive relationships longer due to internal conflict related to what they would potentially lose. The lifelong ties to the land on which many women have grown up is also what they depend on economically (farmland) and plan on pass down to future generations. In addition, the community element of feeling a sense of belonging and connection is also extremely important to many individuals living in small rural and remote communities. Communities in rural, remote, and northern regions are often close knit and depicted as a “rural idyll” (Harvey, 2009). Harvey (2009) defines this term as an ideal place that promotes and reinforces peace, health, home, and family. This term includes the concept that women hold the central role in families and communities. Lastly, the traditional role of the woman ensures the family’s preservation and the moral expectation of self-sacrifice (Cervantes & Sherman, 2021). Wendt and Hornosty (2010) point out the reality of disclosing the abuse or exiting the situation most often results in the woman losing their economic investment (inherited family farm), family, and supports (shunned from community); survivors feel isolated starting over in another location, if that is even viable. Women experiencing abuse may also struggle with posttraumatic stress disorder and/or other mental health concerns (Tutty, 2015). More specifically, the impact of posttraumatic stress disorder and mental health struggles often leads to difficulty accessing social support (withdrawing), lowered self-esteem, and reduced problem-solving skills and advocacy for oneself (Beck et al., 2014). It is important to recognize that women experiencing IPV and DV, who then also experience mental health concerns, are often at an increased risk to return to the abusive relationship (Ford-Gilboe et al., 2015).
The severity of the violence experienced by women in rural, remote, and northern Canada is significantly elevated by the unique factors of isolated geographic locations and rural values. Martz et al. (2016) reports that due to isolated geography the high potential of increased economic poverty often magnifies the severity of IPV. Furthermore, economic dependency, in combination with the increased likelihood or possibility of the perpetrator being unemployed, or engaging in substance abuse, contributes to even higher rates of chronic and severe IPV (Edwards, 2015). Often, those who perpetrate violence may intentionally move their partner to an even more isolated area, away from their established social networks and communities (Dekeseredy & Schwartz, 2009). Finally, lack of access to reliable telephone and internet services, which is often the case outside of urban centres, serves to further enhance social isolation and hinder the ability to seek support services when needed (Moffitt et al., 2020).
Barriers to Support and the Cycle of Violence
It may take multiple attempts to leave an abusive relationship (Griffing et al., 2002) due to the multiplicity of barriers present and the immense difficulty of breaking the cycle of violence. Murray et al. (2015) reports that clinicians working with those attempting to leave abusive relationships call this moment the “window of opportunity.” Khaw and Hardesty (2007) describe this opportunity as a “turning point” that redirects an individual’s path and helps them move from one life stage to another. These turning points are vital for professionals to notice, and are the result of four distinct factors: severity of abuse (e.g., when the individual hits their breaking point), personal resources (e.g. financial independence), social influences (e.g., formal, and informal supports) and child-related influences (e.g. if it is perceived that the children are in danger) (Murray et al., 2015). Other external indicators are education on abuse, informing friends and family members about the past/current abuse, and empowering themselves (e.g. accessing employment opportunities, seeking counselling and other professional services) (Chang et al., 2006).
After Care Support Services
The focus of the helpers supporting the survivor is on their safety and wellbeing. Ford-Gilboe et al. (2015) argue that after the separation, women are in a period of time highlighted by increased potential danger, as a result of financial insecurity, lack of social support, and health risks (Ford-Gilboe et al., 2015), and retaliation by the perpetrator. Financial stress may include suddenly becoming a single parent, childcare costs, transportation costs, finding affordable housing, finding stable employment, or legal costs (Ford-Gilboe et al., 2015). Ford-Gilboe et al. (2015) comment that the lack of social support and health risks include starting over in a new community for safety but without familiarity and social supports, residue of emotional (mental health), and physical impacts (injuries) of the abuse. Finally, helpers should take into consideration that after women exit the violent relationship, the harassment and potential danger of further violence continues or escalates which increases the survivor’s stress levels (Wuest, 2003).
Safety Planning and Assessment
The Ontario Domestic Assault Risk Assessment (ODARA) is a tool that has gained popularity across Canada over the past 10 years. It is the first empirically-tested and validated tool to assess risk of future domestic violence when an assault has already occurred in a relationship, as well as the frequency and severity of the assaults (Hilton et al., 2010). The ODARA asks thirteen questions and each question (historical, current abuse, access to firearms, and assault in pregnancy) reveals a score to look at rates of recidivism (Hilton et al., 2010). Being trained in, and working with, specific risk assessment tools is beneficial for a variety of reasons, including development of a collaborative understanding of the nature of the violence the client is experiencing. The ODARA is an assessment that is accessible for use by police, victim services, social workers, health care, and correctional agencies and enhancing evidence in court (Hilton et al., 2010). The ODARA specifically can inform a client of their overall level of risk, provide information and assistance in taking precautions, and contribute to a safety plan (Hilton et al., 2010).
The choice to leave one’s home is often difficult for individuals who live in rural and remote areas, or for those who live on reserves (Moffitt, 2020) and may include unique obstacles such as the safety of pets or livestock. Research shows that many survivors have strong bonds with their pets (Barrett et al., 2018). However, having a cohesive safety planning template and assessment specific to challenges in rural, remote and northern communities is imperative to ensure continuity of services. Educating RCMP members, healthcare professionals, and community social workers on the cycle of violence, the nature of domestic violence and enhance wrap-around services to support survivors is essential.
While there are several risks that may elevate the potential and severity of violence, one of the most fatal considerations is the access to firearms. Firearms can become weapons of fear, control and violence in intimate partner relationships and studies have revealed that rural families are twice as likely to have access to a firearm and 2.5 times more likely to use a firearm to kill their partner (Banman, 2015). Of the rural, remote, and northern domestic homicides in Canada, 1 in 3 homicides were completed using firearms (Dawson et al., 2018). These types of risks require consideration of safety for the survivor, family and/or the social work practitioner when working in rural, remote, and northern communities.
Further Implications for Social Workers
Social workers working and/or living in rural, remote, and northern communities face unique challenges from their urban practicing counterparts. These factors often include the complexity of client needs without specialized services/specialized trainings (Moffitt et al., 2020), social workers filling multiple roles, lack of available and accessible services/resources (Sandberg, 2013), and the realities of isolation (Wuerch et al., 2019). Other impacts include constantly navigating dual roles with clients and within the community (Turbett, 2009), as well as the lack of anonymity and fearing the person perpetrating the violence may find out about the support given and retaliate against the professional (Ford-Gilboe et al., 2015). These challenges can contribute to a cycle of high turnover and professional burnout of social workers in rural and remote locations (Wuerch et al., 2019).
Micro, Mezzo & Macro Social Work Practice/ Service Delivery
Social workers working in rural, remote, and northern communities are often tasked with engaging in service delivery on multiple levels. Micro social work in communities focuses on engaging with individuals and groups in a therapeutic capacity. Mezzo social work involves a social worker developing and implementing initiatives at a small community level. Macro social work looks more specifically at helping large groups of people through research and policy advocacy and addressing prevalent issues within the community (communities served).
Micro
Social workers in rural, remote, and northern regions who want to create change at the micro level may intervene in diverse ways, such as creating awareness and educational support for individuals, addressing safety concerns, and supporting individuals in accessing services. Edwards (2015) identifies creating awareness of available services by identifying and advertising the services offered in each unique community (e.g. satellite offices, crisis hotlines, etc.). After the first step of creating the initial awareness of available support/services, social workers can support individuals in providing further education (about IPV/DV), pro-actively safety plan (considering all aspects) and help individuals navigate potential barriers to service.
Recommendations for professional practice include increasing anonymity and confidentiality, troubleshooting the lack of transportation, navigating shelters/transitioning houses/safe houses if available (Edwards, 2015), ensuring access to telephone and internet services (Fikowski & Moffitt, n.d.), and engaging in a collaborative process alongside other community services (Pruitt, 2008). Sokoloff and Dupont (2005) advocate for social workers to seek further specialized training when working with women experiencing IPV and DV. Social workers must engage in self-reflective practice so their work can be more effective and considerate of the intersectionalities of each client. Working within rural, remote and northern communities also requires self-reflection to ensure that confidentiality and safety implications and collaborative efforts can be maintained, while also reducing the risk of practitioner burn out.
Mezzo
Research indicates that the community can be a protective factor for women in relation to how the community understands, responds, and prevents IPV (Edwards et al., 2014). Edwards (2015) notes that communities can play a pivotal role in protecting the women in their community through raising awareness of intimate partner violence through public and community education. This awareness, education and coming together begin to shift the dominant harmful narratives in rural communities and may ripple into funding for more intimate partner violence services (volunteer and/or paid) (Edwards, 2015). Social workers can play a crucial role in the community through education, creating community understanding and raising awareness of the prevalence of intimate partner violence in rural, remote and northern communities to ensure that one’s community becomes a protective factor rather than a barrier to accessing supports and services for survivors.
Macro
Rural, remote, and northern communities have varying needs and require voices from these communities to advocate for policy changes related to resource allocation and coordination. Improvements needed include specialized services, safety measures (e.g. shelters), and improved response times. As well, social workers can advocate for improving service response rates for protection orders and increasing resources and funding for IPV intervention and prevention efforts (Edwards, 2015).
Increasing access to affordable housing, transportation, financial security, childcare supports and culturally-appropriate resources is crucial in reducing barriers and stressors that lead to violence (Moffitt et al., 2020).
Finally, it is imperative for social workers and policy makers to work together to shift the cultural norms that support beliefs in traditional gender roles and patriarchy, as well as continuing to educate and increase knowledge about domestic violence, healthy relationships, sexual respect, and the impacts of substance use on families (Barton et al., 2015).
Ethical Considerations
There are a number of ethical considerations for social work practitioners working with survivors of intimate partner violence and domestic violence who practice in rural, remote and northern communities. There are several considerations that a social worker may need to be aware of, such as dual roles which may be defined as when “the social worker interacts in any capacity beyond the worker’s professional role” (Dolgoff et al., 2009). Social workers must engage in reflexive practice regarding the power differential in their relationships. For example, the Canadian Association of Social Workers (CASW, 2005) Code of Ethics speaks directly about the “respect for the inherent dignity and worth of persons” (p. 4) which m ay become increasingly difficult when personal and professional boundaries are blurred (CASW, 2005). In smaller communities, this element can become particularly challenging because members are aware of the multiple roles, and attempt to elicit information, or the community may witness individuals at various social services locations. To provide effective services, social workers practicing in these areas should be cognizant of their boundaries and consider how to navigate their personal and professional lives.
The CASW Code of Ethics (2005) emphasizes the importance of confidentiality and privacy where trust is required for the safety of the client or community. For example, in smaller communities it may be possible that law enforcement or the social worker may be connected with the individual who perpetrated the violence; or anonymity becomes difficult for victims to access support services (Sandberg, 2013). Additionally, research suggests due to the potential lack of anonymity and availability of shelters (if any in or near the community), the perpetrator of violence may easily track down the victim decreasing immediate safety for the victim. (Sandberg, 2013).
As previously discussed, the concept of rurality and maintaining traditional ideals may contribute to further ethical considerations for social workers. Zerbe Enns (2014) highlights that a feminist approach to problems includes two themes, specifically “(1) the personal is political, and (2) problems and symptoms often arise as methods of coping with and surviving in oppressive circumstances” (p. 10). In relation to IPV, this type of perspective shift may be in drastic contrast for a community that may believe IPV is a personal rather than a communal, political, or structural matter.
Social workers practicing in these communities require the ability to be objective and differentiate between objective and subjective perspectives; they likely need to address their biases more frequently than their urban counterparts because of the dual roles they often have. A social worker must be aware of their personal values in relation to the CASW Code of Ethics as there may be competing values and they will need to ensure they are acting in the interest of the client.
Future Implications and Recommendations
In this chapter, we have outlined the importance of intersecting considerations (sex, orientation, ethnicity, rurality), and present challenges with respect to supporting survivors of intimate partner violence in rural, remote and northern communities. Further education, training (e.g., risk assessment), and collaboration between the community and professionals will be pivotal to reducing the impact of violence and the ripple effects in these communities.
Social workers working in these locations need to be cognizant of their own understanding of violence and engage in self-reflexive practice to identify what their community’s needs are so they can advocate in the community and beyond, to stakeholders and policymakers, to cultivate change across all practice levels (micro, macro and mezzo). While this chapter has focused on IPV against women social workers and service providers must have an understanding that IPV and familial violence also impacts other populations (e.g. the 2SLGBTQIA+ communities and heterosexual, cisgender men).
Further recommendations for improving social work interventions and best practice include advocating for improved services in rural, remote, and northern communities to address the current shortage of shelters and support services in rural areas (Barton et al., 2015). To be effective, these services would benefit from addressing the challenges and risk factors specific to rural, remote, and northern communities. Multisector collaboration and coordinated community responses may also help reduce barriers to access in these communities (Eastman et al., 2007). “Wrap around” services for individuals such as shelter services, mental health services, financial support, childcare, housing and transportation support, and education/employment support may also be useful in response to the ever-changing needs of survivors (Eastman et al., 2007). Risk management and safety planning in rural, remote, and northern communities would also benefit from collaboration with police, healthcare, child welfare, victim services, and other social services that can help create a feasible, holistic action plan with the client (Ending Violence Association of B.C., 2021).
Lastly, as future research in this area of concern is conducted, Sandberg (2013) states that researchers should avoid creating a generalized narrative that rural, remote, and northern communities are places of violence. This generalization results in further marginalizing the individuals whom they aim to support (Sokoloff & Dupont, 2005). It is important to understand the oppressive social, colonial, and systemic structures in place that continue to disempower individuals, and to address this detrimental harm in further research, social work practice, and policies and strategies on reporting.
Conclusion
IPV and DV in remote, rural, and northern communities is a significant and ongoing issue. As a social worker working in rural, remote, and northern communities, one is more than likely to encounter IPV at some point during their career. Having a foundational knowledge of IPV, the historical context for DV, and the implications for social workers working with survivors in rural, remote, and northern communities is crucial. Working in collaboration with other professionals and at various practice levels to advocate for social and policy change is necessary to ensure the long-term safety of Canadian women. Further research on the impact and prevalence of women with disabilities and within the 2SLGBTQIA+ community in these geographical contexts will also be crucial in understanding the far-reaching impacts of IPV. Not only do social workers need to collaborate with community members, but federal, provincial, and territorial governments also must begin to work together to challenge the safety of women and vulnerable populations living in rural, remote, and northern communities.
Activities and Assignments
In a small town (i.e. population under 700) located in northern Ontario, Sally lived with her partner, Maliki, her boyfriend of approximately 3 years. Sally is a 22-year-old female who worked part-time at the local grocery store until the birth of her son. Maliki is a 42-year-old general labourer who struggles with maintaining employment and has issues with prescription medications due to a back injury which occurred in his late 20s. In his spare time, Maliki enjoys watching television, fishing, hunting, and knitting. During the first year of their relationship, Maliki had been working consistently; however, he lost his job, and his use of prescription medications increased. Sally then became pregnant. During Sally’s pregnancy, Maliki became quite concerned about money and began controlling the household finances more strictly. When Sally needed money for groceries or bills, Maliki would allot her some cash, although this support often did not cover all the expenses. Financial pressures led to conflicts in their relationship.
When conflicts did arise in their relationship during the first year, there was no violence; however, Maliki would often begin to yell at Sally and then stop talking to her for days or weeks at a time. Then, Sally became pregnant and had a baby boy, Hannigan, who is currently 6-months. In her first trimester, Sally and Maliki had a disagreement and Sally began walking out of the house; Maliki slammed the door, catching Sally’s fingers. The next day, Maliki apologized by taking Sally out for lunch and bringing her flowers. He promised that nothing like that would ever occur again.
As Sally’s pregnancy progressed, Maliki became more concerned about finances and about the upcoming birth. For several months, there were no violent incidents but when Maliki would become angry, he started cleaning his firearms at the kitchen table which made Sally nervous. Sally had attempted to discuss her concern with Maliki, but these conversations often led to conflict; therefore, Sally has not brought up the issue again.
Please answer the following questions in relation to the above case study:
- What are some of the red flags present in this case study?
- With limited resources available in the community, how can you, as the social worker, create a safety plan with Sally?
- What ethical considerations will you need to reflect on?
Additional Resources
- Wuerch, M., Zorn, K., Juschka, D., & Hampton, M. (2019). Responding to intimate partner violence: Challenges faced among service providers in northern communities. Journal of Interpersonal Violence, 34(4), 691–711.
| Types of Abuse |
| Physical Abuse: describes a range of physical contact intended to intimidate, inflict pain and/or bodily harm (Government of Canada, 2019). Psychological Abuse: describes a range of mental tactics to force, manipulate and or control an individual(s) (Government of Canada, 2019). |
| Sexual Abuse: describes involuntary and non-consensual sexual activity obtained either by threats or force (Government of Canada, 2019). |
| Financial Abuse: describes an individual’s access to economic resources controlled by another individual resulting in forced dependence on the perpetrator (Government of Canada, 2019). |
| Neglect: describes a family member who is responsible for another individual but fails to provide basic needs (e.g. shelter, food, medical care, psychological, etc.) (Government of Canada, 2019). |
| Spiritual Abuse: describes abuse perpetrated by trusted spiritual practitioners and/or restrictions and defilement of sacred objects and/or ceremonial practices (Gray et al., 2021). |
| Criminal Harassment & Stalking: describes an individual who repeatedly follows, communicates and/or watches over an individual or an individual’s home for the intent of power and control over a person (Canadian Resource Centre for Victims of Crime, 2011). |
| Cycle of Violence: describes the cyclical, repeating interaction between dichotomous behaviours of abuse and love; tension-building phase, acute/crisis phase and honeymoon phase (Sitter, 2017). |
| The Power and Control Wheel: describes the eight tactics (e.g. coercion/threats, intimidation, emotional abuse, isolation, minimizing/denying/blaming, male privilege, economic abuse) that abusers often use to gain power and control over their victim and which victims often don’t associate as abuse (Cervantes & Sherman, 2021). |
References
Ad Hoc Federal-Provincial-Territorial Working Group. (2017). Final report of the ad hoc federal-provincial-territorial working group reviewing spousal abuse policies and legislation. Government of Canada. https://justice.gc.ca/eng/rp-pr/cj-jp/fv-vf/pol/p2.html
Amnesty International. (2004). Canada: Stolen sisters: A human rights response to discrimination and violence against indigenous women in Canada. https://www.amnesty.org/en/documents/amr20/003/2004/en/
Bandura, A. (1977). Social learning theory. General Learning Press.
Banman, V. (2015). Domestic homicide risk factors: Rural and urban considerations [Master’s thesis, University of Western Ontario]. Electronic Thesis and Dissertation Repository.
Barton, S., Hungler, K., McBride, D., Letourneau, N., & Mailoux, S. (2015). Alberta research project report for provincial stakeholders: Rural and northern community response to intimate partner violence. Faculty of Nursing, University of Alberta.
Barrett, B. J., Fitzgerald, A., Peirone, A., Stevenson, R., & Cheung, C. H. (2018). Help-seeking among abused women with pets: Evidence from a Canadian sample. Victims and Violence, 33(4), 604-626.
Beck, H. G., Clapp, J. D., Jacobs-Lentz, J., McNiff, J., Avery, M., & Olsen, S. A. (2014). The association of mental health conditions with employment, interpersonal, and subjective functioning after intimate partner violence. Violence Against Women, 20(11), 1321-1337.
Bowen, E. A., & Murshid, N. S. (2016). Trauma-informed social policy: A conceptual framework for policy analysis and advocacy. American Journal of Public Health (1971), 106(2), 223-229.
Brassard, R., Montminy, L., Bergeron, A., & Sosa-Sanchez, I. A. (2015). Application of intersectional analysis to data on domestic violence against Aboriginal women living in remote communities in the province of Quebec. Aboriginal Policy Studies, 4(1), 3-23.
Brownridge, D. A. (2008). Understanding the elevated risk of partner violence against Aboriginal women: A comparison of two nationally representative surveys of Canada. Journal of Family Violence, 23(1), 353-367.
Calton, J. M., Cattaneo, L. B., & Gebhard, K. T. (2016). Barriers to help seeking for lesbian, gay, bisexual, transgender, and queer survivors of intimate partner violence. Trauma, Violence & Abuse, 17(5), 585-600.
Campbell, J. C., Webster, D., Koziol-McLain, J., Block, C., Campbell, D., Curry, M. A., Gary, F., Glass, N., McFarlane, J., Sachs, C., Sharps, P., Ulrich, Y., Wilt, S. A., Manganello, J., Xu, X., Schollenberger, J., Frye, V., & Laughon, K. (2003). Risk factors for femicide in abusive relationships: Results from a multisite case control study. American journal of public health, 93(7), 1089–1097.
Canadian Association of Social Workers. (2005). Code Of Ethics. https://www.casw-acts.ca/files/attachements/casw_code_of_ethics.pdf
Canadian Domestic Homicide Prevention Initiative. (2021). Training. Provincial Association of Transition Houses and Services of Saskatchewan. https://pathssk.org/training/
Canadian Resource Centre for Victims of Crime. (2011). Criminal harassment. https://crcvc.ca/docs/Criminal-Harassment-May2011.pdf
Centers for Disease Control and Prevention. (2020). Preventing intimate partner violence. https://www.cdc.gov/violenceprevention/pdf/ipv/IPV-factsheet_2020_508.pdf
Cervantes, M. V., & Sherman, J. (2021). Falling for the ones that were abusive: Cycles of violence in low-income women’s intimate relationships. Journal of Interpersonal Violence, 36(13-14), 7567-7595.
Chang, J. C., Dado, D., Ashton, S., Hawker, L., Cluss, P. A., Buranosky, R., & Scholle, S. H. (2006). Understanding behavior change for women experiencing intimate partner violence: Mapping the ups and downs using the stages of change. Patient Education and Counseling, 62(3), 330–339.
Cohen, D., & Nisbett, R. E. (1994). Self-protection and the culture of honor: Explaining southern violence. Personality & Social Psychology Bulletin, 20(5), 551-567.
Conroy, S. (2021). Family violence in Canada: A statistical profile, 2019. Statistics Canada. https://www150.statcan.gc.ca/n1/en/pub/85-002-x/2021001/article/00001-eng.pdf?st=yWltVh4-
Daoud, N., Smylie, J., Urquia, M., Allan, B., & O’Campo, P. (2013). The contribution of socio-economic position to the excesses of violence and intimate partner violence among Aboriginal versus non-Aboriginal women in Canada. Canadian Journal of Public Health, 104(4), e278-e283.
Dawson, M., Sutton, S., Jaffe, P., Straatman, A., Poon, J., Gosse, M., Peters, O., & Sandhu, G. (2018). One is too many: Trends and patterns in domestic homicides in Canada 2010–2015. Canadian Domestic Homicide Prevention Initiative. http://www.cdhpi.ca/sites/cdhpi.ca/files/CDHPI-REPORTRV_EN.pdf
Dekeseredy, W., & Schwartz, M. D. (2009). Dangerous exists: Escaping abusive relationships in rural America. Rutgers University Press.
Department of Finance Canada. (2021, April 23). Budget 2021: Address by the deputy prime minister and minister of finance. Government of Canada. https://www.canada.ca/en/department-finance/news/2021/04/budget-2021-address-by-the-deputy-prime-minister-and-minister-of-finance.html
Dolgoff, R., Loewenberg, F. M., & Harrington, D. (2009). Ethical decisions for social work practice (8th ed.). Thomson Brooks/Cole.
Eastman, B. J., Bunch, S. G., Williams, A. H., & Carawan, L. W. (2007). Exploring the perceptions of domestic violence service providers in rural localities. Violence Against Women, 13(7), 700-716.
Edwards, K. (2015). Intimate partner violence and the rural–urban–suburban divide: Myth or reality? A critical review of the literature. Trauma, Violence & Abuse, 16(3), 359-373.
Edwards, K. M., Mattingly, M. J., Dixon, K. J., & Banyard, V. L. (2014). Community matters: Intimate partner violence among rural young adults. American Journal of Community Psychology, 53(1), 198-207.
Enns, C. Z. (2004). Feminist theories and feminist psychotherapies: Origins, themes, and diversity (2nd ed.). Routledge.
Fikowski, H., & Moffitt, P. (n.d.). A culture of violence and silence in remote Canada: Impacts on service delivery to address intimate partner violence. In H. Exner-Pirot, B. Norbye, & L. Butler (Eds.), Northern and Indigenous health and healthcare (pp. 198–222). Pressbooks. https://openpress.usask.ca/northernhealthcare/chapter/chapter-15-a-culture-of-violence-and-silence-in-remote-canada-impacts-on-service-delivery-to-address-intimate-partner-violence/
Ford-Gilboe, M., Varcoe, C., Noh, M., West, J., Hammerton, J., Alhalal, E., & Burnett, C. (2015). Patterns and predictors of service use among women who have separated from an abusive partner. Journal of Family Violence, 30(1), 419-431.
Gallup-Black, A. (2005). Rural and urban trends in family and intimate partner homicide in the United States, 1980-1999. Inter-university Consortium for Political and Social Research.
Government of Canada. (n.d.). Family Violence Laws. https://justice.gc.ca/eng/cj-jp/fv-vf/laws-lois.html
Government of Canada. (2019). Abuse: Types of abuse. https://www.canada.ca/en/immigration-refugees-citizenship/corporate/publications-manuals/operational-bulletins-manuals/service-delivery/abuse/types-abuse.html
Government of Canada. (2021a). About family violence. https://www.justice.gc.ca/eng/cj-jp/fv-vf/about-apropos.html
Government of Canada. (2021b). Fact sheet: Intimate partner violence. https://women-gender-equality.canada.ca/en/gender-based-violence-knowledge-centre/intimate-partner-violence.html
Government of Saskatchewan. (2021). Province welcomes RCMP participation, Alberta implementation of “Clare’s Law.” https://www.saskatchewan.ca/government/news-and-media/2021/march/31/province-welcomes-rcmp-participation-alberta-implementation-of-clares-law
Gracia, E. (2004). Unreported cases of domestic violence against women: Towards an epidemiology of social silence, tolerance, and inhibition. Journal of Epidemiology & Community Health, 58(7), 536–537.
Graham, J. R., Shier, M. L., & Delaney, R. (2017). Canadian Social Policy (5th ed.). Pearson Education Canada.
Gray, J., LaBore, K., & Carter, P. (2021). Protecting the sacred tree. Psychology of Religion and Spirituality, 13(2), 204-211.
Griffing, S., Ragin, D. F., Morrison, S. M., Sage, R. E., Madry, L., & Primm, B. J. (2005). Reasons for returning to abusive relationships: Effects of prior victimization. Journal of Family Violence, 20(5), 341-348.
Harvey, D. (2009). Conceptualizing the mental health of rural women: A social work and health promotion perspective. Rural Society, 19(4), 353–362.
Hilton, N. Z., Harris, G. T., & Rice, M. E. (2010). Risk assessment for domestically violent men: Tools for criminal justice, offender intervention and victim services. American Psychological Association.
Howard, J. (2021, January 13). Gender based violence in Canada: Learn the facts. Canadian Women’s Foundation. https://canadianwomen.org/the-facts/gender-based-violence/
Kay, M., & Jeffries, S. (2010). Homophobia, heteronomativism and hegemonic masculinity: Male same-sex intimate partner violence from the perspective of Brisbane service providers. Psychiatry, Psychology and Law, 17(3), 412-423.
Khaw, L., & Hardesty, J. L. (2007). Theorizing the process of leaving: Turning points and trajectories in the stages of change. Family Relations, 56(4), 413-425.
Martz, D. M., Jameson, J. P., & Page, A. D. (2016). Psychological health and academic success in rural Appalachian adolescents exposed to physical and sexual interpersonal violence. American Journal of Orthopsychiatry, 86(5), 594-601.
Moffitt, P., Aujla, W., Giesbrecht, C. J., Grant, I., & Straatman, A. (2020). Intimate partner violence and COVID-19 in rural, remote, and northern Canada: Relationship, vulnerability and risk. Journal of Family Violence.
Moreau, G. (2019). Canadian residential facilities for victims of abuse, 2017/2018. Juristat: Canadian Centre for Justice Statistics, 1-27. https://www150.statcan.gc.ca/n1/en/catalogue/85-002-X201900100007
Murray, C. E., Crowe, A., & Flasch, P. (2015). Turning points: Critical incidents prompting survivors to begin the process of terminating abusive relationships. The Family Journal, 23(1), 228-238.
Murshid, N. S., & Bowen, E. A. (2018). A trauma-informed analysis of the violence against women act’s provisions for undocumented immigrant women. Violence Against Women, 24(13), 1540-1556.
Office of the Chief Coroner Province of Ontario. (2018). Domestic violence death review committee: 2017 annual report. http://cdhpi.ca/sites/cdhpi.ca/files/2017-DVDRC-Report.pdf
Oppal, A. (2012). Forsaken: The report of the missing women commission of inquiry - Volume IIA: Nobodies: How and why we failed the missing and murdered women: Part 1 and 2.Missing Women Commission of Inquiry.
Parliament of Canada. (n.d.). Women’s right to vote in Canada. Retrieved August 18, 2021, from https://lop.parl.ca/sites/ParlInfo/default/en_CA/ElectionsRidings/womenVote
Peterman, L. M., & Dixon, C. G. (2003). Domestic violence between same-sex partners: Implications for counseling. Journal of Counseling & Development, 81(1), 40-47.
Phillips, C. D., & McLeroy, K. R. (2004). Health in rural America: Remembering the importance of place. American Journal of Public Health, 94(10), 1661–1663.
Pruitt, L. R. (2008). Place matters: Domestic violence and rural difference. Wisconsin Journal of Law, Gender & Society, 23(1), 347-419.
Sandberg, L. (2013). Backward, dumb, and violent hillbillies? Rural geographies and intersectional studies on intimate partner violence. Affilia, 28(4), 350-365.
Sitter, K. (2017). Social work with women in Canada: A feminist approach. In S. Hick, & J. Stokes (Eds.), Social work of Canada: An introduction (4th ed., pp. 242-271). Thompson Educational Publishing, Inc.
Sokoloff, N. J., & Dupont, I. (2005). Domestic violence at the intersections of race, class, and gender: Challenges and contributions to understanding violence against marginalized women in diverse communities. Violence Against Women, 11(1), 38–64.
Renzetti, C. M. (1998). Violence and abuse in lesbian relationships: Theoretical and empirical issues. In R. K. Bergen (Ed.), Issues in intimate violence (pp. 117-127). Sage.
Turbett, C. (2009). Tensions in the delivery of social work services in rural and remote Scotland. The British Journal of Social Work, 39(3), 506-521.
Tutty, L. M. (2015). Addressing the safety and trauma issues of abused women: A cross-Canada study of YWCA shelters. Journal of International Women’s Studies, 16(3), 101-116. Bridgewater State College.
United Nations. (n.d.). What is domestic abuse? Retrieved August 16, 2021, from https://www.un.org/en/coronavirus/what-is-domestic-abuse
United Nations Human Rights Office of the High Commissioner. (1993). Declaration on the elimination of violence against women. General Assembly resolution. https://www.ohchr.org/Documents/ProfessionalInterest/eliminationvaw.pdf
Walker, L. E. A. (2002). Politics, psychology and the battered woman's movement. Journal of Trauma Practice, 1(1), 81-102.
Websdale, N., & Johnson, B. (1997). The policing of domestic violence in rural and urban areas: The voices of battered women in Kentucky. Policing & Society, 6(4), 297-317.
Wendt, S., & Hornosty, J. (2010). Understanding contexts of family violence in rural, farming communities: Implications for rural women’s health. Rural Society, 20(1), 51-63.
World Health Organization. (2005). Alcohol and interpersonal violence: Policy briefing. WHO Regional Office for Europe. https://apps.who.int/iris/handle/10665/107351
Women and Gender Equality Canada. (2019). Attitudes regarding gender equality and gender-based violence in Canada: Final report.
World Health Organization. (2011, November 21). WHO: Definition and typology of violence.
Wuest, J., Ford-Gilboe, M., Merritt-Gray, M., & Berman, H. (2003). Intrusion: The central problem for family health promotion among children and single mothers after leaving an abusive partner. Qualitative Health Research, 13(5), 597–622.
Wuerch, M., Zorn, K., Juschka, D., & Hampton, M. (2019). Responding to intimate partner violence: Challenges faced among service providers in northern communities. Journal of Interpersonal Violence, 34(4), 691–711.
The focus of this chapter is on the changing landscape of rural and northern communities in Canada as a result of newcomer settlement in these locations; and on the role of social work in responding to the diverse challenges and opportunities facing these newcomer populations and their receiving communities. The definition of rural and northern being used includes both distance away from the cities or urban centres (spatial) as well as population size of communities (Johnston, 2020; Laurin et al., 2020). The terms settler and immigrant settler are used interchangeably to refer to newcomers who have moved to Canada from other countries. The term “settler” is intentionally used to push readers to keep Canada’s history of colonialism uppermost in mind during the discussions about newcomers in Canada. The chapter recognizes the presence of diasporic peoples who may have once arrived as immigrants but who are now settled as Canadian citizens, and for whom the term “immigrant” is no longer appropriate. This chapter also includes a focus on individuals arriving as refugees who are also seen as newcomers settling in Canada. The chapter recognizes the diverse ways in which newcomers or settlers are able to enter the country (Government of Canada, 2021). The list of pathways includes:
- Express entry (applications are reviewed based on three economic immigration programs: the Federal Skilled Worker, the Federal Skilled Trades Program, and the Canadian Experience Class).
- Family sponsorship
- Provincial Nominee Program
- Quebec-selected skilled workers
- Atlantic immigration pilot
- Caregivers Program
- Start-up Visa (opportunities to start a business or create jobs)
- Self Employment Program
- Rural and Northern Immigration Pilot: (several communities in Alberta, British Columbia, Manitoba, Ontario, and Saskatchewan are participating in this pilot).
- Agri-Food Pilot (opportunities to work in agri-food industries and jobs)
- Health-care workers permanent residence pathway
- Temporary resident to permanent resident pathway
- Permanent residence pathways for Hong Kong residents
In addition to the above, individuals applying as refugees may qualify for entry under the Economic Mobility Pathways Pilot (Government of Canada, n.d.).
The next sections of this chapter will include a brief historical overview of Canada’s newcomer settlement history, followed by a discussion about the implications for social work practice. The discussions on implications for social work practice emphasize the importance of ensuring accessible and culturally relevant services; a focus on the importance of understanding and embracing cultural diversity; the importance of building trusting relationships; and the issue of newcomer settlement within the context of the Truth and Reconciliation Calls to Action.
The chapter emphasizes that social work practice in rural and northern areas offers an array of practice options for social workers: micro, mezzo, and macro because of the complexity of issues.
Learning Objectives
By the end of this chapter you will have had the opportunity to:
- Engage in critical reflection of newcomer settlement history in rural and northern Canada;
- Build knowledge of the complex, intersecting issues experienced by newcomer settlers in rural and northern areas; and
- Reflect on the implications for social work practice with newcomer settlers, in light of the Truth and Reconciliation Calls to Action (Truth and Reconciliation Commission of Canada, 2015).
Background
Immigrant/newcomer settlement in rural and northern Canada has survived despite the growth of industrialization and urbanization which led to the majority of immigrant settlers heading to larger centres such as Toronto, Vancouver, and Montreal (Patel et al., 2019). Provincial Nominee Programs (PNPs) and other policy and program developments have served to bolster settlement in smaller centres, northern, and rural communities across Canada, thereby increasing the diversity in terms of populations and needs. Newcomer settlement has had different impact on different groups of people and communities.
For Indigenous peoples, immigrant/newcomer settlement meant the loss of lands and long-lasting negative impacts on their food security, health and well-being. More specifically, loss of traditional lands resulted in loss of traditional ways of life and in a reliance on European foods (Hossain & Lamb, 2020; Robidoux & Mason, 2017). The long-term impact has been the emergence of physical and mental health challenges among Indigenous peoples in northern and rural communities (Hossain & Lamb, 2020). Indigenous peoples have continued to organize and engage in various strategies to address the historical impact. More recently, the Truth and Reconciliation Commission’s Calls to Action exposed the history of genocide experienced by Indigenous peoples, and provided a comprehensive list of action items to which Canadians are called to respond (Truth and Reconciliation Commission of Canada, 2015).
While immigration policies resulted in losses for Indigenous peoples, they offered the promise of land and prosperity for settlers, many of whom left countries of origin because of economic and social conditions such as violence, poverty and lack of access to land ownership in those countries (Pedersen, 2004). Describing the evolution of immigration policy, Fleras (2014) summarized it as:
Patterns of immigration to Canada corresponded with the changing requirements of its economy. A pre-First World War concentration on agricultural development and domestication of the West gradually segued into a post-Second World War demand for unskilled labour to extract resources or stimulate industrial growth. More recently, emphasis has shifted towards a reliance on highly skilled immigrants as part of a master plan in transitioning towards a global/knowledge economy. (Reitz, 2003; Simmons, 2010, as cited in Fleras, 2014, p. 6)
Many of Canada’s aggressive immigration strategies developed in the 19th century even though settlers had been arriving long before this. The federal government’s early immigration plan initially aimed at attracting White settlers from Britain and Northern Europe to fill labour market needs. The United States was also seen as a viable source country. The promise of employment in infrastructure development (for example, the rail industry) and in agricultural activity was an early attraction, especially in Western Canada (Friesen, 1987; Shepard, 1997). The emergence of settler clusters in rural communities was often facilitated by word of mouth or chain migration. Canada’s ethnic and cultural diversity continued to grow because of the diversity among these settler populations.
Europeans originating from regions outside of Northern Europe experienced racist and discriminatory policies and practices during the early years of Canada’s immigration outreach (Dobrowolsky, 2017). While these latter populations were not immediately welcomed, Canada eventually opened its doors to them. Consequently, a dominant White settler population emerged in rural Canada, with stories of classism, racism, and discrimination affecting these early settler populations in diverse ways, depending on country of origin. The “Whites Only” and/or Whites preferred policies are evidenced by policies, statements, and actions by a long list of Canadian leaders such as Mackenzie King, Wilfrid Laurier, and Robert Borden. Together, these leaders promoted anti-Black, anti-Asian, and other migration strategies and policies in order to limit or restrict settlement populations (Crawford-Holland, 2020; Dobrowolsky, 2017; Niergarth, 2010; Walker, 1985).
Despite the Whites only and/or preferred policies, non-White populations made their way to Canada’s rural and northern communities, also because of the political, social, and economic conditions of source countries. Non-white settlers who were prepared to accept employment as farm or domestic workers were granted entry (Anwar, 2014; Silvera, 1989). Black Americans travelled from the Southern United States of America (USA) to Oklahoma, and then to Canada hoping to find a welcoming country that would offer land and opportunities for a better life (Crawford-Holland, 2020; Walker, 1985). Instead, they encountered a country where systemic racism was embedded within the cultural and social fabric of host communities. Notwithstanding, there are examples of Black settlers setting up successful farms and homesteads in Prairie rural communities such as Amber Valley in Alberta, Maidstone in Saskatchewan, and Swan River in Manitoba (Irby, 1985; Johnsrude, 2004; Shepard, 1997). Canada’s openly racist policies remained in place until 1967 when new immigration regulations were introduced.
The 1967 Immigration Points System introduced changes within immigration policy by placing emphasis on skills, education, and training rather than on factors such as race, ethnicity, and country of origin during the recruitment or screening stage (Anwar, 2014). This Points System reflected a movement away from a focus on agriculture and rural development towards urban development (Verbeeten, 2007). Canada’s 1988 Multiculturalism Act was designed to move the country even further (Berry, 2013). Nevertheless, evolving policies and legislation did not result in the elimination of systemic racism. For example, while the Points System recognized the skills and backgrounds of applicants, this did not necessarily translate into jobs for all newcomers. Canada recruited the brightest and most gifted from developing countries but did not recognize their credentials and out of country work experience when they actually arrived in Canada. Racialized newcomers were often the victims of these discriminatory policies.
More changes were made when provincial nominee programs started emerging after 1998, leading to new immigrant settlement in smaller centres, rural, and northern communities. Nominee programs have provided opportunities for smaller provincial centres, northern, and rural communities to recruit newcomer settlers from varied social, economic, and cultural backgrounds (Bonikowska et al., 2017). Provinces and communities recruited individuals whom they considered to be best suited for their immediate, often short-term needs. Carter et al. (2010) suggest that provinces were usually able to attract newcomers with lower- level skills and/or with specific skill and trades backgrounds. These settlers might not have qualified under the federal skilled worker program. The Northern and Rural Immigration Pilot and the Agri-Food Pilot pathways were launched in 2019. These pathways have offered further opportunities for welcoming communities to attract newcomers to their locations.
Another significant pathway is the temporary foreign worker program which allows employers to hire temporary foreign workers when there are no Canadians available for the jobs. The program includes a focus on highly skilled professionals, seasonal agricultural workers, and domestic workers. The stories of exploitation and abuse of temporary foreign workers are rampant and have been repeatedly raised (Barnetson et al., 2017; Bryan, 2019; Narushima & Sanchez, 2014; Salami et al., 2015). However, these same workers are often reluctant to rock the boat since their participation in the programs and the resultant income are a lifeline for source countries. Families and communities depend on remittances and workers are reluctant to speak out about poor work conditions.
Finally, communities in rural and northern Canada have experienced periods of economic boom and bust, with accompanying employment, economic, and population growth and decline (Dobson et al., 2014; Marchand, 2012). Newcomer settlers have taken advantage of periods of boom and have also experienced the effects of bust. This is particularly relevant to newcomers who moved to northern communities where mining has been occurring (Coderre-Proulx et al., 2016). The arrival, or parachuting in, of newcomers (including interprovincial and international migration) for employment purposes has had significant impact on local communities. In some situations, companies have made investments into local infrastructure, but this has been inconsistent. A study by the Canadian Research Institute for the Advancement of Women described some of the issues facing northern fly-in and fly-out communities (Leung et al., 2016). Many of these communities do not have year-round road access so often depend on air travel. Accommodation may be temporary or portable, and not appropriate for families who are often based elsewhere. In boom times, the arrival of workers and their families in the hub northern or rural communities that serve the mining sites, has resulted in booming opportunities and business for hotels, restaurants, transportation companies, and stores.
At the same time, boom has had other impacts such as skyrocketing rental and housing prices, and challenges for non-mining companies to find workers because these companies are unable to match the high salaries of the mining companies. Those residents who are not employed directly in the mining sector are disadvantaged by the lower wages and skyrocketing prices. Temporary foreign workers employed in the service sector outside of the mining sector are faced with low wages and often overcrowded accommodations. Some research has identified other issues such as women’s vulnerability to violence and an increase in substance abuse issues. An issue that continues to be raised is the impact of mining on the environment, the impact on women and Indigenous communities in the north, and the extent to which dialogue and genuine consultation has been done to identify the impacts of developments on the lives of Indigenous and northern peoples.
The next section will discuss implications for social work practice. The overall message is that the stories and experiences of newcomer settlement are complex and varied. As such, the aim of the section is to encourage students to explore the diverse opportunities that are available to them to address the needs of newcomers in northern and rural communities.
Implications for Social Work Policy and Practice
Overall, stories of life in northern and rural communities offer accounts of tremendous generosity and hope but also provide insight into the extent to which location away from major centres (place/geography) has posed a variety of challenges for newcomer setters and residents in these communities (Burnett et al., 2020; Kulig & Williams, 2011; Patel et al., 2019; Reid, 2019). These challenges include isolation, and unequal access to affordable public transportation, social services, health, and education resources (particularly specialist services). In addition, systemic racism and discrimination continue to be a major issue in communities across Canada.
Social work with newcomer settlers in rural and northern communities therefore offers an array of possibilities for social work practice: direct social work practice, community development, research, advocacy, education, and social policy. The hope is that social workers will engage in practice to support immigrant/refugee/newcomer settlement in these communities, celebrate the strengths of rural and northern communities, and address the disparities experienced as a result of northern and/or rural living.
As noted earlier, immigrant settlement in northern and rural communities has been driven primarily by economic considerations, and by economic and political developments both within source countries and internally in Canada. Immigration patterns and experiences have also been shaped by the talents/expertise that settlers bring to Canada and by government immigrant selection policies (Bonikowska et al., 2017; Kolbe & Kayran, 2019). The end result for communities is the arrival of newcomers from diverse backgrounds including diverse ethno-cultural, professional, educational, language, and class backgrounds. These are important considerations when striving to understand rural and northern immigrant settlement in Canada. The considerations identified above are particularly significant when working to ensure that settlers are able to (1) create a sense of home in their new locations; (2) have access to job and education opportunities that genuinely recognize and credit the credentials, knowledge, and skills which they bring from other countries; (3) have access to culturally relevant and appropriate supports, resources, and services to enhance their settlement and retention in their new locations; and (4) have a sense of well-being that allows them to flourish. They are also relevant issues for social workers who strive to address issues holistically, and who recognize the layered, multidimensional aspects of issues.
Social workers are therefore challenged to remember that a “one size fits all” will not work for newcomer settlers in rural and northern communities. Newcomers may be highly skilled professionals working in the mining and scientific sectors, and they may also be low skilled workers working in lower skilled agricultural or service sector jobs. They may be highly skilled professionals having left situations of violence and extrema trauma. They may be taxi drivers with professional backgrounds who are working other jobs to support families here in Canada and in countries of origin. Social workers will need to develop the knowledge and skills to learn about and understand these diverse realities. As well, communities will need to engage in ongoing reflection, training, and capacity building in order to ensure they are appropriately responsive to the new populations. As discussed in the following sections, policymakers, advocates, and community workers in rural community will need to constantly review, transform, and develop services and resources to respond to the diverse needs of their new arrivants. Areas of concern and need include availability of resources and infrastructure, understanding and embracing cultural diversity, building trusting relationships, and the issue of social work in rural and northern communities in light of the Truth and Reconciliation Calls to Action.
Availability of Resources and Infrastructure
It is worth emphasizing that studies focusing on the retention of newcomer settlers (those arriving as immigrants and refugees) have consistently noted factors such as access to employment (facilitated by recognition of foreign credential and non-Canadian work experience), education, and cultural communities as strong influencers on decisions to remain in communities, or to relocate (Carter et al., 2010; Krahn et al., 2005). Patel et al. (2019)’s scoping review identified factors such as social inclusion, culturally-appropriate services, gender, and housing as distinct social determinants of health factors relevant to well-being in rural and northern communities. Newcomer status adds another layer to these intersecting factors.
More specifically, in addition to generic health and social services, access to formal settlement services (infrastructure) offering language assessment and training programs, employment readiness programs, and mentorship programs have also been identified (Carter et al., 2010; Krahn et al., 2005). Unfortunately, formal settlement infrastructure has not been consistently available in northern and rural areas. Formal infrastructure, which can be seen as sites offering a level of cultural safety, has provided venues where newcomers can reach out to other newcomers and service providers, access resources and support services, raise issues relevant to their settlement needs, and address some of the isolation that they tend to experience. Infrastructure that includes newcomer information centres provides one-stop centres where newcomer immigrant settlers can begin to learn about what services and resources are available in communities. The Northern and Rural Immigration and the Agri-Food Pilots are programs that are well positioned to fill such gaps since they are expected to ensure the availability of settlement and mentoring opportunities for newcomers (Government of Canada, 2021). Many of these welcoming communities already serve as hubs and outreach centres for those living in small towns, on farms, and in other rural locations. The assumption is that these newcomer gateway projects will expand existing resources.
One area where social work intervention would be useful would be to advocate for the development of infrastructure and services that might be missing. This could include advocating for interpreter services for newcomers who are accessing health and education services. Those social workers interested in macro practice could play a leadership role in bringing together various stakeholders to facilitate discussions and research about the development of such services. Another area would be engaging in direct micro practice within settlement agencies, health care, and the schools that newcomer children would be attending. Various communities now have Settlement Worker in School programs (SW1S) as well as social workers who provide a range of referral, support and mentorship services relevant to newcomer children and their families. Finally, social workers in settlement agencies, health, education, and other sectors may choose to engage in group work practice. This would be particularly useful for women who are survivors of abuse and violence; and would be a site where education about issues of violence and abuse could occur. More than anything else, social workers need to have the relevant and appropriate competencies to work well with newcomer women and their families. The next section explores the wide range of personal values and ways of being that all players---- including newcomers, community residents, community workers, and social workers—bring to communities and the relevance of these to successful settlement of newcomers into rural communities.
Understanding and Embracing Cultural Diversity
Newcomers to Canada have tended to move to larger metropolitan centres. As a result, ethnic and cultural diversity of rural and northern communities has evolved at a slower pace than within larger centres. This has been changing over time because of immigration policies, and also because of the emergence of more employment and business opportunities in rural and northern communities. Nevertheless, newcomers are moving into rural and northern communities whose populations may be tightly knit because of longstanding history and well-established relationships (Herron et al., 2021). The same factors that have positive impacts may also include troublesome elements for these populations. Rural residents may have lived in communities for a long time and cultivated a community culture that is slow to change and accept new ideas and ways of being. This reluctance may be driven by a commitment to preserving what is perceived to be dominant, acceptable traditions and cultures.
Those individuals who do not “fit” into the mainstream may include those who are living in poverty, Indigenous peoples, racialized peoples, and gender diverse peoples. Newcomer settler /immigrant/refugee status adds another intersecting dimension, especially when the country of origin is that of a developing country, is not seen to be adequately “Western”, and where English or French (depending on the location) is not the dominant language. Settlement workers, sponsorship groups, and social workers are faced with the challenge of working together to create communities that are open to embracing diversity, equity, and inclusion. This includes facilitating conversations and activities with messages about how diversity will add richness to existing cultures and communities.
In short, newcomers are coming from diverse cultural backgrounds and are living both positive and challenging realities. A huge challenge is to avoid essentializing cultural identity. Essentialist views of identity view identity as singular, fixed and stereotypically applied without paying attention to diversity within cultures and nationalities (Zilliacus et al., 2017). In other situations, there is a tendency to exoticize people of different cultural backgrounds by an over-emphasis on dance, food, and dress (Zilliacus et al., 2017). Social workers are encouraged to engage in critical reflection of the meaning of cultural diversity in order to arrive at a place where they recognize the multiple, rich, evolving, and complex identities of individual newcomers.
Well-intentioned social workers who fail to acknowledge these complexities, add fuel to existing tendencies to demonize or degrade non-Western cultures. For example, lack of acceptance or understanding of non-Christian cultures may lead to Islamophobia. An assumption that Muslim women wearing head coverings are all living in situations of submission fails to recognize the diversity among Muslim women wearing head coverings. In addition, ignorance about the rich cultural heritage of newcomers from many developing countries may lead to patronizing and paternalistic approaches by settlement workers and sponsorship groups. These issues, while common across different geographies, may be particularly problematic in rural and remote regions. Outcomes of ignorance, assumptions of superiority of one culture and way of being over others, and a drive to maintain the resulting status quo are reflected in racism and gender-based discrimination. These issues may be even more intensely felt in rural and northern communities because of geographic location as well as the size of the communities.
There are multiple, interconnected elements to be addressed when seeking to support newcomers in their new homelands, and particularly in northern and rural communities. At the same time, rural and northern communities have well-established traditions of caring for one another. Social workers and other community workers are encouraged to draw on these positive traditions, and play leadership roles in working in partnership with communities to build awareness of the strengths, contributions and complex realities of newcomers. In addition, it is vital that social workers continue to examine their own biases and assumptions throughout their social work careers in order to be part of a process that has positive outcomes for newcomers in rural and northern communities. These actions will go a long way to build trusting relationships that are central to healthy communities.
Building Trusting Relationships
Several studies and reports have exposed the extent to which xenophobia, racism, gender-based discrimination and lack of cultural safety permeate the fabric of rural and northern Canada; and the extent to which these factors have had extensive negative impact on the well-being of communities (Du Mont & Forte, 2016; Higginbottom et al., 2016; Patel et al., 2019; Tungohan, 2017). Higginbottom and others have described how language barriers compromise accessibility to health services. They have also cited examples of newcomer women not understanding the concept of consent or not having faith in service providers’ respect for confidentiality. They comment that newcomer women have not always been able to develop trust and build relationships with service providers because the sessions and processes, including communication styles, are often too fast paced. This results in service users not always understanding or trusting the proposed plans or interventions.
Social workers and other service providers will need to be continually aware of the need to improve their communication skills. This includes paying attention to the pace at which messages are communicated, ensuring the availability of brochures, pamphlets, and messages in multiple languages, and the availability of interpreters and cultural brokers. Of particular note to younger practitioners is to remember to slow down the pace of their speech, without sounding patronizing.
Social workers have a responsibility to ensure that services are relevant and accessible, and that they are able to provide the kinds of services that newcomers will access. Attending workshops and training opportunities to build competency skills will be helpful in building/enhancing communication competency skills for working with newcomers. Engaging in volunteer activities with newcomers in communities and within agencies will serve to build relationships and create visibility and messages of genuine interest and caring to newcomers. These kinds of initiatives will address the longstanding concerns that newcomers do not access mental health support services, even when there are concerns about the need to respond to histories of trauma and the impact on mental health and well-being.
Newcomers in rural and northern communities ought to have access to resources and services similar to those available to residents of larger, urban centres. Social workers and other health care providers recognize the issues of trauma and the accounts of mental illness experienced by many newcomers. However, they are still not always able to provide care because of varied cultural understandings and interpretations of mental illness, which often result in newcomers not accessing services. Other factors include the lack of familiarity with Western models of mental health services, lack of faith in the ability of service providers to respond to their needs, and the issue of stigma associated with mental health. That is, many of the health care needs experienced in urban centres are also prevalent in rural and northern areas. However, communities are now faced with the additional challenge of ensuring the availability of professionals who have the relevant competency skills to work with these diverse newcomer populations.
Technology plays a role in accommodating some of the disparities resulting from geographic distance away from main centres for all citizens. The COVID-19 pandemic highlighted the role of technology such as tele-health and e-health services, and social media tools particularly in rural and northern communities. It also exposed disparities when residents in rural and northern communities experienced unequal access to these same resources and services because of lack of adequate technology infrastructure (bandwidth as an example), and unequal financial resources to access this infrastructure. These are broad issues with which social workers can also be involved.
The above discussions have focused primarily on the role of communities and social workers in providing a welcoming place to newcomers who are arriving from other countries and settling in Canada’s rural and northern regions. Newcomers continue to arrive in Canada at a time when Canadians are grappling with the histories of exclusion, colonization, trauma, genocide, and violence experienced by Indigenous peoples in their own traditional lands. The next section of this chapter emphasizes that ethical social work practice in rural and northern communities requires that social workers learn about the histories of Indigenous peoples, and engage in practice that is grounded in principles of social justice.
Social Work in Rural and Northern Communities within the Context of the Truth and Reconciliation Calls to Action
One of the points raised in the introduction of this chapter is about Canada’s colonial history with Indigenous peoples. The chapter began by noting the loss of land and culture, and the violence experienced by Indigenous peoples. This final section will draw on the United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP) to discuss the role of social work in rural and northern communities within the context of the Truth and Reconciliation Calls to Action (United Nations, 2008). UNDRIP challenges the doctrine of racism and expresses condemnation for the historic injustices suffered during Canada’s colonial rule. The document names the loss of land and resources and applauds the pathways adopted by Indigenous peoples to organize in order to end all forms of discrimination and oppression. It also calls on states to provide prevention measures and redress in response to the colonial history. That is, UNDRIP makes a strong case for social justice. UNDRIP’s declaration of the inherent rights of Indigenous peoples is well aligned with the Social Work Code of Ethics and particularly well synced with value 1: Respect for Inherent Dignity and Worth of People, value 2: Pursuit of Social Justice, and value 3: Service to Humanity. The door is open to social workers engaged with newcomers in rural and northern communities to work with newcomers so that they are immediately engaged in learning about and reflecting on Canada’s colonial history and about the Truth and Reconciliation Commission’s Calls to Action.
The United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP) raises important questions about settler work in mining and extraction industries in particular. How has engagement with Indigenous peoples taken place? Have impact benefit agreements been developed in partnership with Indigenous peoples? (Amyot et al., 2012; Levac & Manning, 2019; Levac et al., 2016). UNDRIP also raises issues about the impact of all developments on the environment and the importance of proactive, consistent discussion with Indigenous people. That is, social workers have an opportunity to work with newcomer settlers so that they are engaged, as fully as possible, in new ways of being with Indigenous peoples. There should not be delay with these kinds of partnerships, teaching opportunities, and dialogue. Some concrete strategies for social workers include facilitating joint attendance at cultural, educational, and social events hosted by Indigenous peoples and newcomer settlers; development of joint social and community activities to build relationships and learn from one another; and facilitating events with attendees from a broad range of backgrounds, including Indigenous individuals and newcomer settlers.
Conclusion
The issues of newcomer settlement in Canada are complex and forever evolving. The pandemic (2019 and beyond) has added complicating factors since Canadians have been required to pay attention to social distancing, to vaccinations, and to doing everything to keep residents safe. This has created an additional burden on social workers who have traditionally worked hard on building human relationships through personal connecting. It has also created stress for communities where personal contacting has always been important. Clearly, technology and social media have helped to respond to the basic human need of connecting with one another. This chapter noted that the pandemic also exposed that not everyone has equal access to the full benefits of technology. This has certainly been the case for northern and rural communities, and will be an area to which policymakers and scientists will continue to attend. Social workers will also need to respond to concerns that not all older adults are comfortable with the use of technology. When immigrant status and language barriers experienced by newcomers are added to the mix, the concerns become more complicated.
The chapter has challenged social workers to understand and embrace cultural diversity and to avoid essentializing cultures and perpetuating assumptions of the superiority of one culture over another. The chapter recognizes the strengths of rural and northern communities and the different ways in which community is built. This includes the sites where community building and dialogue takes place (for example, seniors’ centres, coffee shops and coffee rows, Legion centres, churches, and Elks Halls). The chapter concludes that social workers have a role to play to build bridges between newcomers, residents, and others connected to these locations.
The chapter identifies problematic issues that are present in communities. These include the experiences of temporary foreign workers whose contributions help to sustain communities, but whose experiences of precarity and exploitation are troublesome. These continue to occur at a time when communities are striving to set themselves up as welcoming communities. The chapter also points to Canada’s longstanding history of racism and to the importance of open discussion focused on unraveling root causes in order to address equity and inclusion.
The United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP), along with the Truth and Reconciliation Calls to Action, together provide documents that social workers doing work with newcomers in rural communities can use to facilitate new ways of building relationships and working with Indigenous peoples and Canadian peoples. The documents can also provide important lessons about how to work with newcomer immigrants so that mistakes made with Indigenous peoples, are not repeated by immigrant settlement agencies.
Finally, this chapter recognizes over and over again, the complexities of issues and circumstances relevant to the lives of newcomer immigrant settlers. The chapter recognizes the multiple, intersecting identities of newcomers, and challenges social work students to dive deeper into these and other complex identities and experiences, for example: newcomers with disabilities, newcomers with diverse sexual orientations and gender identities, and newcomers at various life stages. Of particular note for further reflection is the situation of older racialized diasporic adults. These individuals would have come to Canada as immigrants or refugees but are now Canadian citizens. They may have lived as minorities in northern and rural communities for decades and continue to have strong connections to ancestral countries of origin. That is, doing solid, ethical practice with newcomers in Canada’s rural and northern communities calls on social workers to push themselves to be open to the forever changing and complex realities and contexts of these arrivants, settlers, and communities.
Activities and Assignments
- Students are encouraged to locate a settlement agency or immigrant gateway agency in a rural or northern region and discuss the services that are provided. What language supports are available? What services are offered? What is the geographic reach of the agency? What is the general profile of the newcomers they are seeing in their agency? What is the educational background of the workers? How did the community come to have a settlement agency?
- Choose a rural or northern community. What have been the newcomer settler trends over the past 5 years? What might be some of the emerging social issues? What have been the responses? What gaps in services exist? What have been the contributions of the newcomer settlers?
- Students are invited to review the list of communities participating in the Rural and Northern Immigration Pilot and the Agri-Food Pilot. Students are asked to choose two (2) communities to focus on. They are to develop a brief profile of these communities, identify the kinds of newcomer populations that are arriving, and highlight the potential community services that might be required.
References
Amyot, S., Stinson, J., Stienstra, D., & Chansonneuve, D. (2012). Women, economic development & restructuring in Thompson. Canadian Research for the Advancement of Women. https://www.criaw-icref.ca/wp-content/uploads/2021/04/Women-Economic-Development-and-Restructuring-in-Thompson.pdf
Anwar, A. (2014). Canadian immigration policy: Micro and macro issues with the points based assessment system. Canadian Ethnic Studies, 46(1), 169-179.
Barnetson, M., Barnetson, B., & McDonald, S. A. (2017). Farm workers in western Canada: Injustices and activism. University of Alberta Press.
Berry, J. W. (2013). Research on multiculturalism in Canada. International Journal of Intercultural Relations, 37(6), 663-675.
Bonikowska, A., Hou, F., & Picot, G. (2017). New immigrants seeking new places: The role of policy changes in the regional distribution of new immigrants to Canada. Growth and Change, 48(1), 174-190.
Bryan, C. (2019). Labour, population, and precarity: Temporary foreign workers transition to permanent residency in rural Manitoba. Studies in Political Economy, 100(3), 252-269.
Burnett, K., Sanders, C., Halperin, D., & Halperin, S. (2020). Indigenous peoples, settler colonialism, and access to health care in rural and northern Ontario. Health & Place, 66, 102445.
Carter, T., Pandey, M., & Townsend, J. (2010). The Manitoba provincial nominee program: Attraction, integration and retention of immigrants (IRPP Study). Institute for Research on Public Policy.
Coderre-Proulx, M., Campbell, B., & Issiaka Mandé, I. (2016). International migrant workers in the mining sector. International Labour Organization.
Crawford-Holland, S. (2020). The birth of a nation in Canada: Black protest and white denialism across Canada's colour lines. Film History, 32(4), 1-32.
Dobrowolsky, A. (2017). Bad versus big Canada: State imaginaries of immigration and citizenship. Studies in Political Economy, 98(2), 197-222.
Dobson, S., Lemphers, N., & Guilbeault, S. (2014). Booms, busts and bitumen: The economic implications of Canadian oilsands development. The Pembina Institute and Équiterre.
Du Mont, J., & Forte, T. (2016). Perceived discrimination and self-rated health in Canada: An exploratory study. BMC Public Health, 16(1), 742.
Fleras, A. (2014). Immigration Canada: Evolving realities and emerging challenges in a postnational world. UBC Press.
Friesen, G. (1987). The Canadian prairies: A history. University of Toronto Press.
Government of Canada. (2021). Immigrate to Canada. https://www.canada.ca/en/immigration-refugees-citizenship/services/immigrate-canada.html
Government of Canada. (n.d.). Immigrate through the economic mobility pathways pilot: Who is eligible. https://www.canada.ca/en/immigration-refugees-citizenship/services/refugees/economic-mobility-pathways-pilot/immigrate/eligibility.html
Herron, R., Newall, N., Lawrence, B., Ramsey, D., Waddell, C., & Dauphinais, J. (2021). Conversations in times of isolation: Exploring rural-dwelling older adults' experiences of isolation and loneliness during the COVID-19 pandemic in Manitoba, Canada. International Journal of Environmental Research and Public Health, 18(6), 3028.
Higginbottom, G., Safipour, J., Yohani, S., O'Brien, B., Mumtaz, Z., Paton, P., & Barolia, R. (2016). An ethnographic investigation of the maternity healthcare experience of immigrants in rural and urban Alberta, Canada. BMC Pregnancy and Childbirth, 16(1), 20.
Hossain, B., & Lamb, L. (2020). Cultural attachment and wellbeing among Canada’s Indigenous people: A rural urban divide. Journal of Happiness Studies, 21(4), 1303-1324.
Irby, C. C. (1985). Black settlers at Amber Valley, Alberta. The Western Journal of Black Studies, 9(1), 2.
Johnsrude, L. (2004, March 7). Blacks celebrate role in Alberta's settlement: About 1,000 U.S. migrants came in early 1900s. Edmonton Journal.
Johnston, A. (2020). Defining rural teaching hospitals in Canada: Developing and testing a new definition. Canadian Journal of Rural Medicine, 25(4), 1.
Kolbe, M., & Kayran, E. N. (2019). The limits of skill-selective immigration policies. Journal of European Social Policy, 29(4), 478 – 497.
Krahn, H., Derwing, T. M., & Abu-Laban, B. (2005). The retention of newcomers in second- and third- tier Canadian cities. The International Migration Review, 39(4), 872-894.
Kulig, J. C., & Williams, M. (2011). Health in rural Canada. UBC Press.
Laurin, F., Pronovost, S., & Carrier, M. (2020). The end of the urban-rural dichotomy? Towards a new regional typology for SME performance. Journal of Rural Studies, 80, 53-75.
Leung, W., Wilcox, C., White, J., Careen, N., Hutchison, C., & Lake, V. (2016). Fly-in and fly-out communities in Northern Canada. Canadian Research Institute for the Advancement of Women.
Levac, L., & Manning, S. (2019). The importance of Indigenous and Northern women’s experiences and knowledges in impact assessments. Canadian Research Institute for the Advancement of women. https://www.criaw-icref.ca/wp-content/uploads/2021/04/The-Importance-of-Indigenous-and-Northern-Womens-Experiences-and-Knowledges-in-Impact-Assessments.pdf
Levac, L., Manning, S., Stienstra, D., Baikie, G., & Stinson, J. (2016). What do gender and diversity have to do with it? Responding to the community impacts of Canada’s resource development agenda. Canadian Research Institute for the Advancement of women. https://www.criaw-icref.ca/wp-content/uploads/2021/04/What-do-gender-and-diversity-have-to-do-with-it.pdf
Marchand, J. (2012). Local labor market impacts of energy boom-bust-boom in Western Canada. Journal of Urban Economics, 71(1), 165-174.
Narushima, M., & Sanchez, A. (2014). Employers' paradoxical views about temporary foreign migrant workers' health: A qualitative study in rural farms in southern Ontario. International Journal for Equity in Health, 13(1), 65.
Niergarth, K. (2010). ‘This continent must belong to the white races’: William Lyon Mackenzie King, Canadian diplomacy and immigration law, 1908. The International History Review, 32(4), 599-617.
Patel, A., Dean, J., Edge, S., Wilson, K., & Ghassemi, E. (2019). Double burden of rural migration in Canada? Considering the social determinants of health related to immigrant settlement outside the cosmopolis. International Journal of Environmental Research and Public Health, 16(5), 678. https://res.mdpi.com/ijerph/ijerph-16-00678/article_deploy/ijerph-16-00678.pdf
Pedersen, M. (2004). "Wherever two or three are gathered": A study of the Finnish settlement at New Finland, Saskatchewan, 1888-1945 [Master’s thesis, University of Regina]. ProQuest Dissertations and Theses Global.
Reid, S. (2019). The rural determinants of health: Using critical realism as a theoretical framework. Rural and remote health, 19, 5184.
Robidoux, M., & Mason, C. (2017). Introduction. In M. Robidoux & C. Mason (Eds.), A land not forgotten: Indigenous food security and land-based practices in Northern Ontario (pp. 1-15). University of Manitoba Press.
Salami, B., Meharali, S., & Salami, A. (2015). The health of temporary foreign workers in Canada. Canadian Journal of Public Health, 106(8), E546-E554.
Shepard, B. R. (1997). Deemed unsuitable: Blacks from Oklahoma move to the Canadian prairies in search of equality in the early 20th century only to find racism in their new home. Umbrella Press.
Silvera, M. (1989). Silenced: Caribbean domestic workers talk with Makeda Silvera. Sister Vision, Black Women and Women of Colour Press. (Original work published in 1983)
Truth and Reconciliation Commission of Canada. (2015). Truth and Reconciliation Commission of Canada: Calls to action.
Tungohan, E. (2017). From encountering confederate flags to finding refuge in spaces of solidarity: Filipino temporary foreign workers' experiences of the public in Alberta. Space & Polity, 21(1), 11-26.
United Nations. (2008). The United Nations Declaration on the Rights of Indigenous Peoples. Office of the High Commission for Human Rights.
Verbeeten, D. (2007). The past and future of immigration to Canada. Journal of International Migration and Integration, 8(1), 1-10.
Walker, J. (1985). Racial discrimination in Canada: The Black Experience.
Zilliacus, H., Paulsrud, B., & Holm, G. (2017). Essentializing vs. non-essentializing students' cultural identities: Curricular discourses in Finland and Sweden. Journal of Multicultural Discourses, 12(2), 166-180.
In line with a feministic perspective the authors would like to recognize that there is no hierarchy in the contributive efforts of this chapter and acknowledge that this chapter would not have been possible without the differing intersectional perspectives of each author.
Violence against women is still prevalent in Canadian society and directly impacts not only women and their families, but also the collective community. In rural, remote, and northern communities across Canada, pre-existing vulnerabilities and risk of violence against women[1] is increased and often experienced through Intimate Partner Violence (IPV) and Domestic Violence (DV). The frequency of violence against women is a direct reflection of the ongoing social problems in Canada resulting in the inequality of women (e.g., historical, social, political, cultural, and economic, etc.). Conroy (2021) identifies that in 2019, the rates of family violence in remote and rural Canadian communities was 2.0 times higher than in the rest of Canada, and intimate partner violence was 1.8 times higher in rural and remote communities.
While these statistics are concerning, Gracia (2004) suggests that the majority of IPV and DV against women often goes unreported due to a multiplicity of societal oppression(s), personal circumstances, and barriers to accessing support. However, those who live with multiple intersectional ties may be at a higher risk of violence, particularly Indigenous, immigrant, and Lesbian/Bisexual/Transgender/Intersex (LBTI) women living in rural, remote, and northern regions (Calton et al., 2016; Daoud et al., 2013; Murshid & Bowen, 2018).
This chapter focuses on IPV against women in rural, remote, and northern regions. However, it should be noted that while women may also perpetuate violence, that will not be the focus of this chapter. Furthermore, it provides an opportunity to learn and reflect on the prevalence of IPV and DV in rural, remote, and northern communities within Canada and how social work practitioners support the work being done at the micro, mezzo, and macro levels. Social workers providing services in these communities need to be aware of risks, how to provide risk assessment, and how to incorporate safety considerations for those who may be experiencing IPV and DV.
[1] In this chapter the term “woman/women” refers to cisgender, trans, intersex, and anyone identifying as a “woman.”
Learning Objectives
By the end of this chapter, the following learning objectives should be achieved:
- Understanding of definitions of IPV and DV and awareness of the rates and the historical context for this issue in Canada, specifically in rural, remote and northern communities
- Awareness of implications for social workers working with victims of IPV and DV in rural, remote, and northern communities across Canada
- Understanding of specific safety planning and practice considerations for social work professionals on a micro, mezzo, and macro level
- Awareness of the importance for social workers to develop collaborative working relationships, and educational and advocacy opportunities to reduce the severity and frequency of IPV and DV occurrences.
Theoretical Framework
The complexity of violence and its impact may be best understood through a feminist, trauma-informed, intersectional lens. In alignment with a feminist perspective, this chapter uses the term “survivor,” rather than “victim,” as the word “victim” pathologizes and disempowers the woman who has experienced violence (Walker, 2002). Feminist theology serves to empower women and raise awareness that disparity and oppression within larger, structural, and political systems exist (Corbeil et al., 1983, as cited in Walker, 2002). In combination with a trauma-informed lens, principles grounding our understanding of domestic violence include the following: safety, trustworthiness and transparency, collaboration and peer support, empowerment, and choice for survivors (Bowen & Murshid, 2016). Applying these principles in understanding violence, in order to support survivors, highlights a useful approach to providing care that is not re-traumatizing. In addition, using an intersectional lens allows individuals to gain a deeper understanding of IPV and DV. For example, Sokoloff and Dupont (2005) explain that violence experienced and reflected among an individual’s social locators (e.g., culture) may be interpreted by the survivor differently than by witnesses or observers. Therefore, it is important to be aware that cultural differences should not mask the larger systemic and structural forms of oppression (e.g. racism, colonialism, sexism, heterosexism, ableism, patriarchy, economic exploitation, etc.) that impact and increase violence for women across diverse social locators (Sokoloff & Dupont, 2005).
History of Domestic Violence in Rural, Remote and Northern Communities
Canada is a vast country, with most of its population residing in large urban cities (Moffitt et al., 2020) and an estimated 19% of Canadians in rural and remote areas (Statistics Canada, as cited in Graham et al., 2017). Historically, the violence perpetrated against women has been embedded in many institutions and remains entrenched covertly and overtly in our current systems. For example, the women’s suffrage movement and resistance against the dominant, patriarchal Canadian society began in Manitoba in 1916 (Parliament of Canada, n.d.). Other provinces, such as Saskatchewan and Alberta, followed suit until, on a federal platform, Canada conceded to the pressures of change (Parliament of Canada, n.d.). However, while there were a number of significant changes and rights acknowledged in the 20th century, violence against women continues to be a significant issue (Sitter, 2017). Walker (2002) highlights that during the 1970s, a network of shelters was developed across North America in response to violence against women (Government of Canada, 2021b).
Service Delivery
The delivery of safety services for survivors of IPV continues to be an area of advocacy research/development and ongoing evaluation for social workers in Canada. While DV does not differentiate among geographical locations, social workers working in rural, remote and northern areas of Canada have unique service delivery needs and limitations based on resources and location. The implementation of IPV policies that have been developed and implemented in more densely populated areas of Canada are often inadequate in meeting the needs of rural, remote, and northern communities.
Policy
Policy development for IPV and DV continues to be an area of concern, since several Canadian provinces lack legislation to support the survivors of violence. In 2021, six provinces (Alberta, Manitoba, Newfoundland and Labrador, Nova Scotia, Prince Edward Island and Saskatchewan) and three territories had implemented legislation to support survivors of IPV, in addition to the laws set forth in the Canadian Criminal Code (Government of Canada, 2021b). The Criminal Code is meant to prohibit some forms of IPV, including “physical and sexual assault, some forms of emotional/psychological abuse and neglect, and financial abuse” (Government of Canada, 2021a, para. 3); however, further support is required to address intimate partner violence (IPV) across Canada.
As part of the Canadian Advisory Council on the Status of Women’s work conducted in 1980, there were key changes and suggestions made and implemented in the Criminal Code to address the issue of IP V at the time (Ad Hoc Federal-Provincial-Territorial Working Group, 2017). Other examples include an amendment in 1983 to protect partners in their intimate relationships from such acts as spousal rape, and in 1993 to include criminal harassment (i.e., stalking) (Government of Canada, 2021b). More recently,
…in June 2019, the Criminal Code was amended to strengthen the criminal justice’s response to IPV, including by defining ‘intimate partner’ for all Criminal Code purposes and clarifying that the term includes a current or former spouse, common-law partner and dating partner. (Government of Canada, 2021b, para. 5)
With that said, between 1974 and 2001, there was a 62% decrease of spousal homicides, suggesting that many of the changes had the desired effect (Ad Hoc Federal-Provincial-Territorial Working Group, 2017).
Provincial policymakers have continued to address the issue of IPV in provinces, such as in Saskatchewan where rates are above the national average, by developing legislation such as the Interpersonal Violence Disclosure Protocol “Clare’s Law” (Government of Saskatchewan, 2021). First implemented in Britain in 2014, Clare’s Law has been adopted, not only by the vast majority of municipal police in cities across Saskatchewan, but also more recently by the RCMP (Canadian Domestic Homicide Prevention Initiative, 2021; Government of Saskatchewan, 2021). With Clare’s Law, an applicant can make a request regarding access to information about an individual’s history and past criminal charges which may be disclosed by the proper authorities if they believe that the person they are disclosing to is currently at risk (Canadian Domestic Homicide Prevention Initiative, 2021). These policy changes provide increased safety options for survivors of violence and promote choice and empowerment for survivors in collaboration with social workers and RCMP/police professionals.
The Impact of Domestic Violence
Not only is IPV and DV devastating for the survivor of the relationship, but its implications are also far reaching and may affect the entire family, particularly if children and/or adolescents are living in the family home. IPV also has impact on communities (large and small) and can be particularly devastating when combined with factors that further enhance the vulnerability of individuals and communities.
Childhood & Adolescence
As researchers, organizations and frontline staff who work with women and children who experience IPV and DV, there is an emphasis on interventions and prevention strategies. Cervantes and Sherman (2021) state that early exposure to violence in the home increases the chances that the cycle of violence will continue later in life for those children. Repeated witnessing of these behaviours normalizes this interaction, and children further learn this behaviour by imitating what they observe (Bandura, 1997). Therefore, exposure to violence in the home may increase a child’s risk of expecting, engaging in, and tolerating violent behaviour in their own intimate relationships, thus continuing the cycle of violence intergenerationally (Cervantes & Sherman, 2021). The schemas developed by children and adolescents in terms of intimate relationships are often replicated, unless an individual is exposed to a new environment, which can then become a catalyst for change (Cervantes & Sherman, 2021). Martz et al. (2016) note that their research demonstrated that rural adolescents were at an increased risk for physical and sexual violence with their intimate partners, when compared to urban adolescents. This research is troubling as rural adolescents, and adults, have even less access to information, social supports, and formal services in their communities.
First Nations, Metis & Inuit Women
Colonialism has damaged and changed traditional cultural beliefs in First Nation, Metis and Inuit communities towards women. Daoud et al. (2013) note that before colonialism, women in these cultural communities held respected and valued roles, and it was unthinkable to engage in violence against women. Conroy (2021) identifies that due to historical and ongoing colonialism in Canada, IPV is a direct result of compounding factors such as residential schools, the 60s Scoop, the child welfare system, and murdered and missing Indigenous women. These factors can combine in creating intergenerational trauma, addiction, and poverty, as well as enforcing traditional, euro-centric, christian gender roles on Indigenous women (Daoud et al., 2013). Studies demonstrate that rates of violence are considerably higher among Indigenous women, especially in rural and remote areas in Canada (Brownridge, 2008) where Indigenous women experience IPV eight times more than non-Indigenous women (Daoud et al., 2013). In consideration of these disturbing statistics, Moreau (2019) notes that in 2017/2018 there were 522 domestic violence shelters across Canada, and only 30 of these shelters located on reserves. Daoud et al. (2013) argues that due to colonization, violence was introduced and still impacts the community in multiple ways. The first is through collective violence in the form of institutional discrimination that attacks human rights for Indigenous communities. The next is forcing patriarchal and Christian values onto Indigenous communities resulting in a shift in their gender roles and the balance of power among genders. The third distinction is a result of colonial policies, such as residential schools. Intergenerational trauma was perpetrated with the removal of children from their families, communities and culture, and the experience of abuse (physical/emotional/sexual/cultural) while in care. Intergenerational trauma from childhood experiences often results in family and intimate partner violence later in children’s lives.
The violence continues to be so pervasive that campaigns, such as Amnesty International’s Stolen Sisters, have been initiated to increase awareness around the higher rates of violence and discrimination perpetrated against First Nations women (Amnesty International, 2004). Statistics suggest that this group is six times more likely to be killed (Howard, 2021), and Oppal (2012) reported that First Nations, Metis, and Inuit women represent 10% of all female homicides, which is significantly disproportionate compared to the overall national crime rate against women.
Indigenous women living in remote, rural, and northern communities in Canada can also face significant barriers to leaving an abusive relationship, such as not wanting to leave one’s family community or reserve (Campbell et al., 2003), limited or no access to a shelter, lack of support, and the cost of travel. These compounding challenges, combined with intergenerational trauma, contributes to ongoing colonialism in First Nations communities. Elders tell stories of the impact of colonization, the introduction of alcohol and disease, and the mistreatment of women (Moffitt et al., 2020). According to the World Health Organization (WHO), alcohol consumption can further increase the risk for IPV. For example, excessive use of alcohol was identified as a risk factor for intimate partner homicide in 40% of cases reviewed in Ontario between 2003 and 2017 (Office of the Chief Coroner Province of Ontario, 2018).
Newcomers to Canada
Another vulnerable population to consider in rural, remote, and northern locations is newcomers to Canada. These women face further unique barriers when living in these regions, such as discrimination (e.g. racism), culture shock, communication (e.g. language) and immigration status (Ford-Gilboe et al., 2015; Murshid & Bowen, 2018; Sandberg, 2013; Sokoloff & Dupont, 2005). While many immigrant and refugee women experience barriers, these women are often dependent on their partners who perpetuate the abuse (Sandberg, 2013). This dependency may include financial dependency (education in other countries may not transfer), isolation from the cultural community, understanding IPV laws in Canada (Murshid & Bowen, 2018), lack of awareness of services (Ford-Gilboe et al., 2015), and the inability to leave the current home (Sandberg, 2013). The individuals perpetrating violence gain power and control by exploiting threats of deportation, reinforcement of patriarchal gender roles and relationships, and fear of losing custody of their children (Murshid & Bowen, 2018). Leaving the relationship is difficult due to discrimination experienced from a variety of sources including consideration of housing options and police involvement (Murshid & Bowen, 2018). Police may be under-educated or hold immigration bias/racist beliefs and may view the violence as a cultural attribute (Sokoloff & Dupont, 2005).
Lesbian, Bisexual, Transgender, and Intersex (LBTI) Women
One major unique barrier facing women in the Lesbian, Bisexual, Trans and Intersex (LBTI) community is a lack of knowledge and information possessed by service providers regarding LBTI issues and various forms of discrimination connected with this intersectionality. Kay and Jefferies (2010) explain that due to our heteronormative society, the classical definition and understanding of IPV is that a woman is harmed by a male. Furthermore, the two spirited, lesbian, gay, bi-sexual, transgender, queer, intersex and a-sexual plus (2SLGBTQIA+) community education around IPV is insufficient and 2SLGBTQIA+ individuals experiencing IPV may not classify their experiences as violence due to dominant cultural templates (Calton et al., 2016). Further, education in this area for professionals is severely lacking. Survivors seeking help may encounter further discrimination and stigma by law enforcement, the court system, and by helping professionals (e.g. homo/bi/transphobia), which may result in returning to their abuser and/or not reporting or seeking help for future occurrences (Calton et al., 2016; Sokoloff & Dupont, 2005). Renzetti (1998) notes the complexity that internalized homophobia plays as a contributing factor, as the survivor fears disclosing the violence. LBTI perpetrators of violence use internalized homophobia and the fear of discrimination by service providers and the community to gain more power and control over their partners (Sokoloff & Dupont, 2005). They often use the tactic of threatening to “out” their partner (Sokoloff & Dupont, 2005), and emphasize the potential risk of losing one’s children, employment, relationships (family/friends/community) or housing (Calton et al., 2016). Peterman and Dixon (2003) identified that if shelters are available for LBTI users, there is a unique risk that the perpetrator may enter the “safe” space (i.e. shelter) and commit further abuse and/or harass their partner. As well, service providers or residents at these shelters may be homo/bi/transphobic making them unsafe (Sokoloff & Dupont, 2005).
Barriers to Service Delivery
Due to the complexity and multilevel experiences of oppression, Murray et al. (2015) note that women often do not make an immediate decision to leave a violent partner/situation after a single incident; it is usually after gradual increases in violence that survivors make this decision. Furthermore, survivors of intimate partner violence and domestic violence will often leave and later return to their partner who perpetrated abuse multiple times before leaving for good (Murray et al., 2015). To begin understanding the barriers that face women living in rural, remote, and northern geographies experiencing IPV and DV, we suggest that social workers reflect on the four levels of oppression that are involved: societal/cultural, institutional, interpersonal, and personal.
Societal and Cultural
Sexism, patriarchy, Catholicism, racism and traditional “family values” still affect the lives of Canadian women. These oppressive ideologies often are more prominent and reinforced in rural communities. Wendt and Hornosty (2010) state that patriarchal attitudes, gender stereotypes, traditional family units, and traditional gender roles are interwoven with rural values. These large oppressive structures and ideologies trickle down and reinforce violence against women which can make it difficult for them to leave abusive situations in rural, remote, and northern communities.
The impact of COVID-19 on IPV and DV situations has also added an additional layer of complexity for women. Women who were experiencing IPV/DV before and into the pandemic were further isolated from opportunities/resources as health orders for public safety iterated stay home orders and physical distancing. Fears of exposure to the virus, not being able to access shelters, and feeling the need to stay home with their partners prevented many survivors from reaching out during this time (Moffitt et al., 2020). Survivors who were already isolated due to geographical location had a decrease in chances that a neighbour might potentially overhear/witness or intervene during a violent episode (Sandberg, 2013), and a new barrier was thus created by the virus with the narrative that isolation equals safety (Moffitt et al., 2020). In addition, the impact of the pandemic with factors of higher stress levels on individuals and families (e.g., partners losing work, children’s remote learning) led to increased risk for controlling behaviors and/or heightened barriers for accessing support (Moffitt et al., 2020).
Institutional
Women living in rural, remote, and northern communities face further oppression as the societal beliefs recur within institutions, and survivors encounter unique barriers due to the geographical location they reside in. Research shows that many rural communities pride themselves on “moral lifestyles,” including the sanctity of marriage, family life, and Christian- centered values that serve as the foundation of their town. For example, the institution of marriage impacts survivors of IPV and DV; Cervantes and Sherman (2021) conclude that many women believe that the abuse they encounter is a consequence of marriage. This patriarchal belief instills in women the conviction that, due to their decision to marry (“for better or for worse”), they must endure the abuse no matter how violent the experience. Furthermore, Wendt and Hornosty (2010) comment that in rural life, masculine power and privilege is publicly visible. This privilege is often seen in farming organizations, bars, municipal governments, and sports teams. In terms of local municipal government, Edwards (2015) comments that in certain rural, remote and northern communities, individuals in power may hold the belief that IPV is non-existent and therefore less government involvement in providing preventative or crisis services is needed.
Women experiencing IPV and DV living in rural, remote, and northern locations face increased difficulty accessing services than their urban counterparts. These services may include daycare, community resources, law enforcement (Edwards, 2015), transportation, social services, courts, and shelters (Sandberg, 2013). Services are frequently lacking and limited due to lower population density than is needed to create or receive funding (Phillips & McLeroy, 2004), and the information regarding services is not easily accessible. If services are available, barriers may include issues related to privacy and anonymity, poverty (Edwards, 2015), lack of response from service providers due to long waitlists, being placed on a waitlist, difficulty getting information (Ford-Gilboe et al., 2015), and geographical isolation from community and social support (Sandberg, 2013). Sandberg (2013) notes that the often-low socioeconomic reality of isolated communities results in lack of infrastructure, poor road conditions, lack of job opportunities, and fewer voluntary supports. Regarding law enforcement, Websdale and Johnson (1997) found that rural law enforcement had longer wait times when called and individuals were lucky if police even showed up regarding DV situations. This delay in time-sensitive support and medical care in rural, remote, and northern communities results in increased risk of homicide, due the severity of the inflicted injuries (Gallup-Black, 2005). Additionally, specialized services ranging from police, lawyers, social supports, local courts, and judges often lacked specialized training in IPV and DV (Sandberg, 2013).
Interpersonal
Cervantes and Sherman (2021) identify that, within rural, remote and northern contexts, a commonly-held belief is that domestic violence is not a community problem/responsibility but a personal issue that should remain private. Cohen and Nisbetter (1994) emphasize that rural communities pride themselves on a “culture of honor” which stays quiet and accepts violence, especially if it puts a family’s reputation at risk. This self-preservation at the community level, with the additional barriers of geographic location, makes it difficult for women to find support or resources. Dekeseredy and Schwartz (2009) identify that a safety risk more specific to rural communities occurs when the individual who perpetuates violence has high social capital and, as a result, the likelihood of the tight-knit community supporting the woman is low. Regarding safety, Sandberg (2013) comments that in rural life, conflicts of interest and anonymity are almost non-existent. Law enforcement, social workers, and medical professionals are likely to have a personal relationship with the individual who perpetuates abuse, and safe houses may be difficult to keep invisible from that individual.
Personal
Identity for rural women becomes a potential barrier to services, as Wendt and Hornosty (2010) state that many rural women who have a strong identity with the land, community, and preservation of the family may stay in abusive relationships longer due to internal conflict related to what they would potentially lose. The lifelong ties to the land on which many women have grown up is also what they depend on economically (farmland) and plan on pass down to future generations. In addition, the community element of feeling a sense of belonging and connection is also extremely important to many individuals living in small rural and remote communities. Communities in rural, remote, and northern regions are often close knit and depicted as a “rural idyll” (Harvey, 2009). Harvey (2009) defines this term as an ideal place that promotes and reinforces peace, health, home, and family. This term includes the concept that women hold the central role in families and communities. Lastly, the traditional role of the woman ensures the family’s preservation and the moral expectation of self-sacrifice (Cervantes & Sherman, 2021). Wendt and Hornosty (2010) point out the reality of disclosing the abuse or exiting the situation most often results in the woman losing their economic investment (inherited family farm), family, and supports (shunned from community); survivors feel isolated starting over in another location, if that is even viable. Women experiencing abuse may also struggle with posttraumatic stress disorder and/or other mental health concerns (Tutty, 2015). More specifically, the impact of posttraumatic stress disorder and mental health struggles often leads to difficulty accessing social support (withdrawing), lowered self-esteem, and reduced problem-solving skills and advocacy for oneself (Beck et al., 2014). It is important to recognize that women experiencing IPV and DV, who then also experience mental health concerns, are often at an increased risk to return to the abusive relationship (Ford-Gilboe et al., 2015).
The severity of the violence experienced by women in rural, remote, and northern Canada is significantly elevated by the unique factors of isolated geographic locations and rural values. Martz et al. (2016) reports that due to isolated geography the high potential of increased economic poverty often magnifies the severity of IPV. Furthermore, economic dependency, in combination with the increased likelihood or possibility of the perpetrator being unemployed, or engaging in substance abuse, contributes to even higher rates of chronic and severe IPV (Edwards, 2015). Often, those who perpetrate violence may intentionally move their partner to an even more isolated area, away from their established social networks and communities (Dekeseredy & Schwartz, 2009). Finally, lack of access to reliable telephone and internet services, which is often the case outside of urban centres, serves to further enhance social isolation and hinder the ability to seek support services when needed (Moffitt et al., 2020).
Barriers to Support and the Cycle of Violence
It may take multiple attempts to leave an abusive relationship (Griffing et al., 2002) due to the multiplicity of barriers present and the immense difficulty of breaking the cycle of violence. Murray et al. (2015) reports that clinicians working with those attempting to leave abusive relationships call this moment the “window of opportunity.” Khaw and Hardesty (2007) describe this opportunity as a “turning point” that redirects an individual’s path and helps them move from one life stage to another. These turning points are vital for professionals to notice, and are the result of four distinct factors: severity of abuse (e.g., when the individual hits their breaking point), personal resources (e.g. financial independence), social influences (e.g., formal, and informal supports) and child-related influences (e.g. if it is perceived that the children are in danger) (Murray et al., 2015). Other external indicators are education on abuse, informing friends and family members about the past/current abuse, and empowering themselves (e.g. accessing employment opportunities, seeking counselling and other professional services) (Chang et al., 2006).
After Care Support Services
The focus of the helpers supporting the survivor is on their safety and wellbeing. Ford-Gilboe et al. (2015) argue that after the separation, women are in a period of time highlighted by increased potential danger, as a result of financial insecurity, lack of social support, and health risks (Ford-Gilboe et al., 2015), and retaliation by the perpetrator. Financial stress may include suddenly becoming a single parent, childcare costs, transportation costs, finding affordable housing, finding stable employment, or legal costs (Ford-Gilboe et al., 2015). Ford-Gilboe et al. (2015) comment that the lack of social support and health risks include starting over in a new community for safety but without familiarity and social supports, residue of emotional (mental health), and physical impacts (injuries) of the abuse. Finally, helpers should take into consideration that after women exit the violent relationship, the harassment and potential danger of further violence continues or escalates which increases the survivor’s stress levels (Wuest, 2003).
Safety Planning and Assessment
The Ontario Domestic Assault Risk Assessment (ODARA) is a tool that has gained popularity across Canada over the past 10 years. It is the first empirically-tested and validated tool to assess risk of future domestic violence when an assault has already occurred in a relationship, as well as the frequency and severity of the assaults (Hilton et al., 2010). The ODARA asks thirteen questions and each question (historical, current abuse, access to firearms, and assault in pregnancy) reveals a score to look at rates of recidivism (Hilton et al., 2010). Being trained in, and working with, specific risk assessment tools is beneficial for a variety of reasons, including development of a collaborative understanding of the nature of the violence the client is experiencing. The ODARA is an assessment that is accessible for use by police, victim services, social workers, health care, and correctional agencies and enhancing evidence in court (Hilton et al., 2010). The ODARA specifically can inform a client of their overall level of risk, provide information and assistance in taking precautions, and contribute to a safety plan (Hilton et al., 2010).
The choice to leave one’s home is often difficult for individuals who live in rural and remote areas, or for those who live on reserves (Moffitt, 2020) and may include unique obstacles such as the safety of pets or livestock. Research shows that many survivors have strong bonds with their pets (Barrett et al., 2018). However, having a cohesive safety planning template and assessment specific to challenges in rural, remote and northern communities is imperative to ensure continuity of services. Educating RCMP members, healthcare professionals, and community social workers on the cycle of violence, the nature of domestic violence and enhance wrap-around services to support survivors is essential.
While there are several risks that may elevate the potential and severity of violence, one of the most fatal considerations is the access to firearms. Firearms can become weapons of fear, control and violence in intimate partner relationships and studies have revealed that rural families are twice as likely to have access to a firearm and 2.5 times more likely to use a firearm to kill their partner (Banman, 2015). Of the rural, remote, and northern domestic homicides in Canada, 1 in 3 homicides were completed using firearms (Dawson et al., 2018). These types of risks require consideration of safety for the survivor, family and/or the social work practitioner when working in rural, remote, and northern communities.
Further Implications for Social Workers
Social workers working and/or living in rural, remote, and northern communities face unique challenges from their urban practicing counterparts. These factors often include the complexity of client needs without specialized services/specialized trainings (Moffitt et al., 2020), social workers filling multiple roles, lack of available and accessible services/resources (Sandberg, 2013), and the realities of isolation (Wuerch et al., 2019). Other impacts include constantly navigating dual roles with clients and within the community (Turbett, 2009), as well as the lack of anonymity and fearing the person perpetrating the violence may find out about the support given and retaliate against the professional (Ford-Gilboe et al., 2015). These challenges can contribute to a cycle of high turnover and professional burnout of social workers in rural and remote locations (Wuerch et al., 2019).
Micro, Mezzo & Macro Social Work Practice/ Service Delivery
Social workers working in rural, remote, and northern communities are often tasked with engaging in service delivery on multiple levels. Micro social work in communities focuses on engaging with individuals and groups in a therapeutic capacity. Mezzo social work involves a social worker developing and implementing initiatives at a small community level. Macro social work looks more specifically at helping large groups of people through research and policy advocacy and addressing prevalent issues within the community (communities served).
Micro
Social workers in rural, remote, and northern regions who want to create change at the micro level may intervene in diverse ways, such as creating awareness and educational support for individuals, addressing safety concerns, and supporting individuals in accessing services. Edwards (2015) identifies creating awareness of available services by identifying and advertising the services offered in each unique community (e.g. satellite offices, crisis hotlines, etc.). After the first step of creating the initial awareness of available support/services, social workers can support individuals in providing further education (about IPV/DV), pro-actively safety plan (considering all aspects) and help individuals navigate potential barriers to service.
Recommendations for professional practice include increasing anonymity and confidentiality, troubleshooting the lack of transportation, navigating shelters/transitioning houses/safe houses if available (Edwards, 2015), ensuring access to telephone and internet services (Fikowski & Moffitt, n.d.), and engaging in a collaborative process alongside other community services (Pruitt, 2008). Sokoloff and Dupont (2005) advocate for social workers to seek further specialized training when working with women experiencing IPV and DV. Social workers must engage in self-reflective practice so their work can be more effective and considerate of the intersectionalities of each client. Working within rural, remote and northern communities also requires self-reflection to ensure that confidentiality and safety implications and collaborative efforts can be maintained, while also reducing the risk of practitioner burn out.
Mezzo
Research indicates that the community can be a protective factor for women in relation to how the community understands, responds, and prevents IPV (Edwards et al., 2014). Edwards (2015) notes that communities can play a pivotal role in protecting the women in their community through raising awareness of intimate partner violence through public and community education. This awareness, education and coming together begin to shift the dominant harmful narratives in rural communities and may ripple into funding for more intimate partner violence services (volunteer and/or paid) (Edwards, 2015). Social workers can play a crucial role in the community through education, creating community understanding and raising awareness of the prevalence of intimate partner violence in rural, remote and northern communities to ensure that one’s community becomes a protective factor rather than a barrier to accessing supports and services for survivors.
Macro
Rural, remote, and northern communities have varying needs and require voices from these communities to advocate for policy changes related to resource allocation and coordination. Improvements needed include specialized services, safety measures (e.g. shelters), and improved response times. As well, social workers can advocate for improving service response rates for protection orders and increasing resources and funding for IPV intervention and prevention efforts (Edwards, 2015).
Increasing access to affordable housing, transportation, financial security, childcare supports and culturally-appropriate resources is crucial in reducing barriers and stressors that lead to violence (Moffitt et al., 2020).
Finally, it is imperative for social workers and policy makers to work together to shift the cultural norms that support beliefs in traditional gender roles and patriarchy, as well as continuing to educate and increase knowledge about domestic violence, healthy relationships, sexual respect, and the impacts of substance use on families (Barton et al., 2015).
Ethical Considerations
There are a number of ethical considerations for social work practitioners working with survivors of intimate partner violence and domestic violence who practice in rural, remote and northern communities. There are several considerations that a social worker may need to be aware of, such as dual roles which may be defined as when “the social worker interacts in any capacity beyond the worker’s professional role” (Dolgoff et al., 2009). Social workers must engage in reflexive practice regarding the power differential in their relationships. For example, the Canadian Association of Social Workers (CASW, 2005) Code of Ethics speaks directly about the “respect for the inherent dignity and worth of persons” (p. 4) which m ay become increasingly difficult when personal and professional boundaries are blurred (CASW, 2005). In smaller communities, this element can become particularly challenging because members are aware of the multiple roles, and attempt to elicit information, or the community may witness individuals at various social services locations. To provide effective services, social workers practicing in these areas should be cognizant of their boundaries and consider how to navigate their personal and professional lives.
The CASW Code of Ethics (2005) emphasizes the importance of confidentiality and privacy where trust is required for the safety of the client or community. For example, in smaller communities it may be possible that law enforcement or the social worker may be connected with the individual who perpetrated the violence; or anonymity becomes difficult for victims to access support services (Sandberg, 2013). Additionally, research suggests due to the potential lack of anonymity and availability of shelters (if any in or near the community), the perpetrator of violence may easily track down the victim decreasing immediate safety for the victim. (Sandberg, 2013).
As previously discussed, the concept of rurality and maintaining traditional ideals may contribute to further ethical considerations for social workers. Zerbe Enns (2014) highlights that a feminist approach to problems includes two themes, specifically “(1) the personal is political, and (2) problems and symptoms often arise as methods of coping with and surviving in oppressive circumstances” (p. 10). In relation to IPV, this type of perspective shift may be in drastic contrast for a community that may believe IPV is a personal rather than a communal, political, or structural matter.
Social workers practicing in these communities require the ability to be objective and differentiate between objective and subjective perspectives; they likely need to address their biases more frequently than their urban counterparts because of the dual roles they often have. A social worker must be aware of their personal values in relation to the CASW Code of Ethics as there may be competing values and they will need to ensure they are acting in the interest of the client.
Future Implications and Recommendations
In this chapter, we have outlined the importance of intersecting considerations (sex, orientation, ethnicity, rurality), and present challenges with respect to supporting survivors of intimate partner violence in rural, remote and northern communities. Further education, training (e.g., risk assessment), and collaboration between the community and professionals will be pivotal to reducing the impact of violence and the ripple effects in these communities.
Social workers working in these locations need to be cognizant of their own understanding of violence and engage in self-reflexive practice to identify what their community’s needs are so they can advocate in the community and beyond, to stakeholders and policymakers, to cultivate change across all practice levels (micro, macro and mezzo). While this chapter has focused on IPV against women social workers and service providers must have an understanding that IPV and familial violence also impacts other populations (e.g. the 2SLGBTQIA+ communities and heterosexual, cisgender men).
Further recommendations for improving social work interventions and best practice include advocating for improved services in rural, remote, and northern communities to address the current shortage of shelters and support services in rural areas (Barton et al., 2015). To be effective, these services would benefit from addressing the challenges and risk factors specific to rural, remote, and northern communities. Multisector collaboration and coordinated community responses may also help reduce barriers to access in these communities (Eastman et al., 2007). “Wrap around” services for individuals such as shelter services, mental health services, financial support, childcare, housing and transportation support, and education/employment support may also be useful in response to the ever-changing needs of survivors (Eastman et al., 2007). Risk management and safety planning in rural, remote, and northern communities would also benefit from collaboration with police, healthcare, child welfare, victim services, and other social services that can help create a feasible, holistic action plan with the client (Ending Violence Association of B.C., 2021).
Lastly, as future research in this area of concern is conducted, Sandberg (2013) states that researchers should avoid creating a generalized narrative that rural, remote, and northern communities are places of violence. This generalization results in further marginalizing the individuals whom they aim to support (Sokoloff & Dupont, 2005). It is important to understand the oppressive social, colonial, and systemic structures in place that continue to disempower individuals, and to address this detrimental harm in further research, social work practice, and policies and strategies on reporting.
Conclusion
IPV and DV in remote, rural, and northern communities is a significant and ongoing issue. As a social worker working in rural, remote, and northern communities, one is more than likely to encounter IPV at some point during their career. Having a foundational knowledge of IPV, the historical context for DV, and the implications for social workers working with survivors in rural, remote, and northern communities is crucial. Working in collaboration with other professionals and at various practice levels to advocate for social and policy change is necessary to ensure the long-term safety of Canadian women. Further research on the impact and prevalence of women with disabilities and within the 2SLGBTQIA+ community in these geographical contexts will also be crucial in understanding the far-reaching impacts of IPV. Not only do social workers need to collaborate with community members, but federal, provincial, and territorial governments also must begin to work together to challenge the safety of women and vulnerable populations living in rural, remote, and northern communities.
Kristie Panchuk (she/her) is a Cisgender, Female, White Settler, Able-bodied, registered clinical social worker (SK)
Curtis Hart (he/him) is a queer, male, mixed ancestry, registered social worker (BC).
Dillion Lewchuk (he/him) is a queer, male, white settler, disabled, able-bodied, therapist (BC)
Activities and Assignments
In a small town (i.e. population under 700) located in northern Ontario, Sally lived with her partner, Maliki, her boyfriend of approximately 3 years. Sally is a 22-year-old female who worked part-time at the local grocery store until the birth of her son. Maliki is a 42-year-old general labourer who struggles with maintaining employment and has issues with prescription medications due to a back injury which occurred in his late 20s. In his spare time, Maliki enjoys watching television, fishing, hunting, and knitting. During the first year of their relationship, Maliki had been working consistently; however, he lost his job, and his use of prescription medications increased. Sally then became pregnant. During Sally’s pregnancy, Maliki became quite concerned about money and began controlling the household finances more strictly. When Sally needed money for groceries or bills, Maliki would allot her some cash, although this support often did not cover all the expenses. Financial pressures led to conflicts in their relationship.
When conflicts did arise in their relationship during the first year, there was no violence; however, Maliki would often begin to yell at Sally and then stop talking to her for days or weeks at a time. Then, Sally became pregnant and had a baby boy, Hannigan, who is currently 6-months. In her first trimester, Sally and Maliki had a disagreement and Sally began walking out of the house; Maliki slammed the door, catching Sally’s fingers. The next day, Maliki apologized by taking Sally out for lunch and bringing her flowers. He promised that nothing like that would ever occur again.
As Sally’s pregnancy progressed, Maliki became more concerned about finances and about the upcoming birth. For several months, there were no violent incidents but when Maliki would become angry, he started cleaning his firearms at the kitchen table which made Sally nervous. Sally had attempted to discuss her concern with Maliki, but these conversations often led to conflict; therefore, Sally has not brought up the issue again.
Please answer the following questions in relation to the above case study:
- What are some of the red flags present in this case study?
- With limited resources available in the community, how can you, as the social worker, create a safety plan with Sally?
- What ethical considerations will you need to reflect on?
Additional Resources
- Wuerch, M., Zorn, K., Juschka, D., & Hampton, M. (2019). Responding to intimate partner violence: Challenges faced among service providers in northern communities. Journal of Interpersonal Violence, 34(4), 691–711.
| Types of Abuse |
| Physical Abuse: describes a range of physical contact intended to intimidate, inflict pain and/or bodily harm (Government of Canada, 2019). Psychological Abuse: describes a range of mental tactics to force, manipulate and or control an individual(s) (Government of Canada, 2019). |
| Sexual Abuse: describes involuntary and non-consensual sexual activity obtained either by threats or force (Government of Canada, 2019). |
| Financial Abuse: describes an individual’s access to economic resources controlled by another individual resulting in forced dependence on the perpetrator (Government of Canada, 2019). |
| Neglect: describes a family member who is responsible for another individual but fails to provide basic needs (e.g. shelter, food, medical care, psychological, etc.) (Government of Canada, 2019). |
| Spiritual Abuse: describes abuse perpetrated by trusted spiritual practitioners and/or restrictions and defilement of sacred objects and/or ceremonial practices (Gray et al., 2021). |
| Criminal Harassment & Stalking: describes an individual who repeatedly follows, communicates and/or watches over an individual or an individual’s home for the intent of power and control over a person (Canadian Resource Centre for Victims of Crime, 2011). |
| Cycle of Violence: describes the cyclical, repeating interaction between dichotomous behaviours of abuse and love; tension-building phase, acute/crisis phase and honeymoon phase (Sitter, 2017). |
| The Power and Control Wheel: describes the eight tactics (e.g. coercion/threats, intimidation, emotional abuse, isolation, minimizing/denying/blaming, male privilege, economic abuse) that abusers often use to gain power and control over their victim and which victims often don’t associate as abuse (Cervantes & Sherman, 2021). |
References
Ad Hoc Federal-Provincial-Territorial Working Group. (2017). Final report of the ad hoc federal-provincial-territorial working group reviewing spousal abuse policies and legislation. Government of Canada. https://justice.gc.ca/eng/rp-pr/cj-jp/fv-vf/pol/p2.html
Amnesty International. (2004). Canada: Stolen sisters: A human rights response to discrimination and violence against indigenous women in Canada. https://www.amnesty.org/en/documents/amr20/003/2004/en/
Bandura, A. (1977). Social learning theory. General Learning Press.
Banman, V. (2015). Domestic homicide risk factors: Rural and urban considerations [Master’s thesis, University of Western Ontario]. Electronic Thesis and Dissertation Repository.
Barton, S., Hungler, K., McBride, D., Letourneau, N., & Mailoux, S. (2015). Alberta research project report for provincial stakeholders: Rural and northern community response to intimate partner violence. Faculty of Nursing, University of Alberta.
Barrett, B. J., Fitzgerald, A., Peirone, A., Stevenson, R., & Cheung, C. H. (2018). Help-seeking among abused women with pets: Evidence from a Canadian sample. Victims and Violence, 33(4), 604-626.
Beck, H. G., Clapp, J. D., Jacobs-Lentz, J., McNiff, J., Avery, M., & Olsen, S. A. (2014). The association of mental health conditions with employment, interpersonal, and subjective functioning after intimate partner violence. Violence Against Women, 20(11), 1321-1337.
Bowen, E. A., & Murshid, N. S. (2016). Trauma-informed social policy: A conceptual framework for policy analysis and advocacy. American Journal of Public Health (1971), 106(2), 223-229.
Brassard, R., Montminy, L., Bergeron, A., & Sosa-Sanchez, I. A. (2015). Application of intersectional analysis to data on domestic violence against Aboriginal women living in remote communities in the province of Quebec. Aboriginal Policy Studies, 4(1), 3-23.
Brownridge, D. A. (2008). Understanding the elevated risk of partner violence against Aboriginal women: A comparison of two nationally representative surveys of Canada. Journal of Family Violence, 23(1), 353-367.
Calton, J. M., Cattaneo, L. B., & Gebhard, K. T. (2016). Barriers to help seeking for lesbian, gay, bisexual, transgender, and queer survivors of intimate partner violence. Trauma, Violence & Abuse, 17(5), 585-600.
Campbell, J. C., Webster, D., Koziol-McLain, J., Block, C., Campbell, D., Curry, M. A., Gary, F., Glass, N., McFarlane, J., Sachs, C., Sharps, P., Ulrich, Y., Wilt, S. A., Manganello, J., Xu, X., Schollenberger, J., Frye, V., & Laughon, K. (2003). Risk factors for femicide in abusive relationships: Results from a multisite case control study. American journal of public health, 93(7), 1089–1097.
Canadian Association of Social Workers. (2005). Code Of Ethics. https://www.casw-acts.ca/files/attachements/casw_code_of_ethics.pdf
Canadian Domestic Homicide Prevention Initiative. (2021). Training. Provincial Association of Transition Houses and Services of Saskatchewan. https://pathssk.org/training/
Canadian Resource Centre for Victims of Crime. (2011). Criminal harassment. https://crcvc.ca/docs/Criminal-Harassment-May2011.pdf
Centers for Disease Control and Prevention. (2020). Preventing intimate partner violence. https://www.cdc.gov/violenceprevention/pdf/ipv/IPV-factsheet_2020_508.pdf
Cervantes, M. V., & Sherman, J. (2021). Falling for the ones that were abusive: Cycles of violence in low-income women’s intimate relationships. Journal of Interpersonal Violence, 36(13-14), 7567-7595.
Chang, J. C., Dado, D., Ashton, S., Hawker, L., Cluss, P. A., Buranosky, R., & Scholle, S. H. (2006). Understanding behavior change for women experiencing intimate partner violence: Mapping the ups and downs using the stages of change. Patient Education and Counseling, 62(3), 330–339.
Cohen, D., & Nisbett, R. E. (1994). Self-protection and the culture of honor: Explaining southern violence. Personality & Social Psychology Bulletin, 20(5), 551-567.
Conroy, S. (2021). Family violence in Canada: A statistical profile, 2019. Statistics Canada. https://www150.statcan.gc.ca/n1/en/pub/85-002-x/2021001/article/00001-eng.pdf?st=yWltVh4-
Daoud, N., Smylie, J., Urquia, M., Allan, B., & O’Campo, P. (2013). The contribution of socio-economic position to the excesses of violence and intimate partner violence among Aboriginal versus non-Aboriginal women in Canada. Canadian Journal of Public Health, 104(4), e278-e283.
Dawson, M., Sutton, S., Jaffe, P., Straatman, A., Poon, J., Gosse, M., Peters, O., & Sandhu, G. (2018). One is too many: Trends and patterns in domestic homicides in Canada 2010–2015. Canadian Domestic Homicide Prevention Initiative. http://www.cdhpi.ca/sites/cdhpi.ca/files/CDHPI-REPORTRV_EN.pdf
Dekeseredy, W., & Schwartz, M. D. (2009). Dangerous exists: Escaping abusive relationships in rural America. Rutgers University Press.
Department of Finance Canada. (2021, April 23). Budget 2021: Address by the deputy prime minister and minister of finance. Government of Canada. https://www.canada.ca/en/department-finance/news/2021/04/budget-2021-address-by-the-deputy-prime-minister-and-minister-of-finance.html
Dolgoff, R., Loewenberg, F. M., & Harrington, D. (2009). Ethical decisions for social work practice (8th ed.). Thomson Brooks/Cole.
Eastman, B. J., Bunch, S. G., Williams, A. H., & Carawan, L. W. (2007). Exploring the perceptions of domestic violence service providers in rural localities. Violence Against Women, 13(7), 700-716.
Edwards, K. (2015). Intimate partner violence and the rural–urban–suburban divide: Myth or reality? A critical review of the literature. Trauma, Violence & Abuse, 16(3), 359-373.
Edwards, K. M., Mattingly, M. J., Dixon, K. J., & Banyard, V. L. (2014). Community matters: Intimate partner violence among rural young adults. American Journal of Community Psychology, 53(1), 198-207.
Enns, C. Z. (2004). Feminist theories and feminist psychotherapies: Origins, themes, and diversity (2nd ed.). Routledge.
Fikowski, H., & Moffitt, P. (n.d.). A culture of violence and silence in remote Canada: Impacts on service delivery to address intimate partner violence. In H. Exner-Pirot, B. Norbye, & L. Butler (Eds.), Northern and Indigenous health and healthcare (pp. 198–222). Pressbooks. https://openpress.usask.ca/northernhealthcare/chapter/chapter-15-a-culture-of-violence-and-silence-in-remote-canada-impacts-on-service-delivery-to-address-intimate-partner-violence/
Ford-Gilboe, M., Varcoe, C., Noh, M., West, J., Hammerton, J., Alhalal, E., & Burnett, C. (2015). Patterns and predictors of service use among women who have separated from an abusive partner. Journal of Family Violence, 30(1), 419-431.
Gallup-Black, A. (2005). Rural and urban trends in family and intimate partner homicide in the United States, 1980-1999. Inter-university Consortium for Political and Social Research.
Government of Canada. (n.d.). Family Violence Laws. https://justice.gc.ca/eng/cj-jp/fv-vf/laws-lois.html
Government of Canada. (2019). Abuse: Types of abuse. https://www.canada.ca/en/immigration-refugees-citizenship/corporate/publications-manuals/operational-bulletins-manuals/service-delivery/abuse/types-abuse.html
Government of Canada. (2021a). About family violence. https://www.justice.gc.ca/eng/cj-jp/fv-vf/about-apropos.html
Government of Canada. (2021b). Fact sheet: Intimate partner violence. https://women-gender-equality.canada.ca/en/gender-based-violence-knowledge-centre/intimate-partner-violence.html
Government of Saskatchewan. (2021). Province welcomes RCMP participation, Alberta implementation of “Clare’s Law.” https://www.saskatchewan.ca/government/news-and-media/2021/march/31/province-welcomes-rcmp-participation-alberta-implementation-of-clares-law
Gracia, E. (2004). Unreported cases of domestic violence against women: Towards an epidemiology of social silence, tolerance, and inhibition. Journal of Epidemiology & Community Health, 58(7), 536–537.
Graham, J. R., Shier, M. L., & Delaney, R. (2017). Canadian Social Policy (5th ed.). Pearson Education Canada.
Gray, J., LaBore, K., & Carter, P. (2021). Protecting the sacred tree. Psychology of Religion and Spirituality, 13(2), 204-211.
Griffing, S., Ragin, D. F., Morrison, S. M., Sage, R. E., Madry, L., & Primm, B. J. (2005). Reasons for returning to abusive relationships: Effects of prior victimization. Journal of Family Violence, 20(5), 341-348.
Harvey, D. (2009). Conceptualizing the mental health of rural women: A social work and health promotion perspective. Rural Society, 19(4), 353–362.
Hilton, N. Z., Harris, G. T., & Rice, M. E. (2010). Risk assessment for domestically violent men: Tools for criminal justice, offender intervention and victim services. American Psychological Association.
Howard, J. (2021, January 13). Gender based violence in Canada: Learn the facts. Canadian Women’s Foundation. https://canadianwomen.org/the-facts/gender-based-violence/
Kay, M., & Jeffries, S. (2010). Homophobia, heteronomativism and hegemonic masculinity: Male same-sex intimate partner violence from the perspective of Brisbane service providers. Psychiatry, Psychology and Law, 17(3), 412-423.
Khaw, L., & Hardesty, J. L. (2007). Theorizing the process of leaving: Turning points and trajectories in the stages of change. Family Relations, 56(4), 413-425.
Martz, D. M., Jameson, J. P., & Page, A. D. (2016). Psychological health and academic success in rural Appalachian adolescents exposed to physical and sexual interpersonal violence. American Journal of Orthopsychiatry, 86(5), 594-601.
Moffitt, P., Aujla, W., Giesbrecht, C. J., Grant, I., & Straatman, A. (2020). Intimate partner violence and COVID-19 in rural, remote, and northern Canada: Relationship, vulnerability and risk. Journal of Family Violence.
Moreau, G. (2019). Canadian residential facilities for victims of abuse, 2017/2018. Juristat: Canadian Centre for Justice Statistics, 1-27. https://www150.statcan.gc.ca/n1/en/catalogue/85-002-X201900100007
Murray, C. E., Crowe, A., & Flasch, P. (2015). Turning points: Critical incidents prompting survivors to begin the process of terminating abusive relationships. The Family Journal, 23(1), 228-238.
Murshid, N. S., & Bowen, E. A. (2018). A trauma-informed analysis of the violence against women act’s provisions for undocumented immigrant women. Violence Against Women, 24(13), 1540-1556.
Office of the Chief Coroner Province of Ontario. (2018). Domestic violence death review committee: 2017 annual report. http://cdhpi.ca/sites/cdhpi.ca/files/2017-DVDRC-Report.pdf
Oppal, A. (2012). Forsaken: The report of the missing women commission of inquiry - Volume IIA: Nobodies: How and why we failed the missing and murdered women: Part 1 and 2.Missing Women Commission of Inquiry.
Parliament of Canada. (n.d.). Women’s right to vote in Canada. Retrieved August 18, 2021, from https://lop.parl.ca/sites/ParlInfo/default/en_CA/ElectionsRidings/womenVote
Peterman, L. M., & Dixon, C. G. (2003). Domestic violence between same-sex partners: Implications for counseling. Journal of Counseling & Development, 81(1), 40-47.
Phillips, C. D., & McLeroy, K. R. (2004). Health in rural America: Remembering the importance of place. American Journal of Public Health, 94(10), 1661–1663.
Pruitt, L. R. (2008). Place matters: Domestic violence and rural difference. Wisconsin Journal of Law, Gender & Society, 23(1), 347-419.
Sandberg, L. (2013). Backward, dumb, and violent hillbillies? Rural geographies and intersectional studies on intimate partner violence. Affilia, 28(4), 350-365.
Sitter, K. (2017). Social work with women in Canada: A feminist approach. In S. Hick, & J. Stokes (Eds.), Social work of Canada: An introduction (4th ed., pp. 242-271). Thompson Educational Publishing, Inc.
Sokoloff, N. J., & Dupont, I. (2005). Domestic violence at the intersections of race, class, and gender: Challenges and contributions to understanding violence against marginalized women in diverse communities. Violence Against Women, 11(1), 38–64.
Renzetti, C. M. (1998). Violence and abuse in lesbian relationships: Theoretical and empirical issues. In R. K. Bergen (Ed.), Issues in intimate violence (pp. 117-127). Sage.
Turbett, C. (2009). Tensions in the delivery of social work services in rural and remote Scotland. The British Journal of Social Work, 39(3), 506-521.
Tutty, L. M. (2015). Addressing the safety and trauma issues of abused women: A cross-Canada study of YWCA shelters. Journal of International Women’s Studies, 16(3), 101-116. Bridgewater State College.
United Nations. (n.d.). What is domestic abuse? Retrieved August 16, 2021, from https://www.un.org/en/coronavirus/what-is-domestic-abuse
United Nations Human Rights Office of the High Commissioner. (1993). Declaration on the elimination of violence against women. General Assembly resolution. https://www.ohchr.org/Documents/ProfessionalInterest/eliminationvaw.pdf
Walker, L. E. A. (2002). Politics, psychology and the battered woman's movement. Journal of Trauma Practice, 1(1), 81-102.
Websdale, N., & Johnson, B. (1997). The policing of domestic violence in rural and urban areas: The voices of battered women in Kentucky. Policing & Society, 6(4), 297-317.
Wendt, S., & Hornosty, J. (2010). Understanding contexts of family violence in rural, farming communities: Implications for rural women’s health. Rural Society, 20(1), 51-63.
World Health Organization. (2005). Alcohol and interpersonal violence: Policy briefing. WHO Regional Office for Europe. https://apps.who.int/iris/handle/10665/107351
Women and Gender Equality Canada. (2019). Attitudes regarding gender equality and gender-based violence in Canada: Final report.
World Health Organization. (2011, November 21). WHO: Definition and typology of violence.
Wuest, J., Ford-Gilboe, M., Merritt-Gray, M., & Berman, H. (2003). Intrusion: The central problem for family health promotion among children and single mothers after leaving an abusive partner. Qualitative Health Research, 13(5), 597–622.
Wuerch, M., Zorn, K., Juschka, D., & Hampton, M. (2019). Responding to intimate partner violence: Challenges faced among service providers in northern communities. Journal of Interpersonal Violence, 34(4), 691–711.
Photos taken by Kaity Inookee and Emma Akulukjuk-Hackett on September 18, 2021
Consistent with other remote Indigenous communities, social work in Nunavut has many unique challenges and limitations. The current chapter aims to explore and understand approaches to these challenges, through the introduction of a case study highlighting common realities across Nunavut. We will further describe several practice approaches and competencies in navigating the case study. As social workers, we must understand the historical and social complexities of Inuit populations to consider any approach or intervention in the provision of service. It is our hope that the introduction of Inuit history and its context will enrich your approach to care within our region. We introduce and explain the Child Advocacy Centre (CAC) model, which works within the Inuit Qaujimajatuqangit (IQ) principles. We will also explain the Umingmak CAC and how its introduction has changed the response to childhood trauma within our jurisdiction, and allowed for more inter-departmental communication and collaboration. This change has ultimately shifted the response to care of our most vulnerable children and adolescents in our community.
This chapter will review Inuit history, values, community response to supporting children and adolescents with disclosures, as well as challenges, barriers and interventions. Although the content may seem extensive, we recognize that it may still not feel complete in capturing the complexity of social work in Nunavut. As a future social worker, you need to immerse yourself in the content while maintaining a critical lens of the larger impact of colonialism on service provision. The chapter might also illicit certain reactions based on your own social location and your beliefs about how service delivery should look or be implemented. If you find yourself challenged at certain moments, manage the discomfort as you are able and then return to the chapter when you are ready.
Learning Objectives
This chapter will focus on the following elements that will serve to inform the learning objectives:
- Historical context of Inuit in the Arctic
- Inuit societal values
- Community response to care
- Child Advocacy Centres
- Multidisciplinary teams
- Ethical considerations
- Barriers and challenges
Inuit history from pre-colonialism to current realities will be reviewed. We acknowledge that we are not Inuit and do not represent Inuit. We write about Inuit culture and heritage only to assist in the description of unique social work practice in our location. We encourage you to look to Inuit organizations and individuals for further information on this subject. Our intention is to provide some foundational understanding relating to themes of distrust in service provision caused by colonialism. Inuit societal values will be explored in the context of resilience and the sustaining of Inuit traditions. Inuit societal values are integral to policy enactment and subsequently service provision. The review of values will add another layer of learning about the strength of Inuit. As an emerging social worker, your understanding of a community response to care is integral to service provision. At times, you may feel disconnected from the theory as realities of practice crystalize; you are encouraged to challenge your learning during this process. We will review community response to care in our Inuit community and the complexity of service provision. Child Advocacy Centres (CAC) have been transformative in many communities with respect to service provision for children and adolescents who have disclosed distinct forms of maltreatment. Therefore, we will review the history of CACs and the impact in communities, particularly Nunavut.
A part of Inuit societal values relates to working together for a common good. This value is explored through a discussion about working in multidisciplinary teams. As social workers we are actively confronted with ethical dilemmas, and these can be unique in remote communities such as Nunavut where your neighbour might also be your client. Attention to ethical considerations in small communities will be explored. We will conclude our learning by discussing barriers and challenges experienced by social workers in Nunavut. In particular, the section will highlight some of the progress relating to service delivery but will also review a call to action in highlighting the challenges ahead. Prior to our learning on Inuit history, to provide additional context to social work in Nunavut, please review the case study of Jessica, which will guide this chapter.
Case Study of Jessica
This fictitious case study of Jessica will focus on the realities of remote communities, such as service pathways for those located in Nunavut. The authors aim to highlight specific challenges faced as a result of this context.
Jessica is a 10-year-old Inuk girl who is currently in grade 5 in Kinngait, Nunavut. Jessica has three younger siblings and resides with them and her mother (Tapisa) within a multigenerational household that is owned by her uncle (Jamesie); there are 11 people residing in the three bedroom home. Tapisa has a history of alcohol dependence but in the past year has focused on her personal healing. The former partner (Peter) of Tapisa died by suicide when Jessica was 5 years old.
A couple of years ago, Tapisa started working as a machine operator for a mining company. Tapisa works in another fly-in community on a three-week rotation and then is home for three weeks. During the time Tapisa is away working, Jessica and her siblings are cared for by extended family members within the home.
During a recent outburst in the home by Jessica, Tapisa took her daughter aside to help regulate her. Jessica disclosed to her mother that she was being sexually abused by one of her uncles during the period that Tapisa was working at the mining company. Jessica pointed to pain in her vaginal area. Tapisa was very shocked and emotional with her daughter. Tapisa reassured her daughter that she was safe, thanked her for telling her, and assured her that she would deal with it.
Tapisa took Jessica to the Community Health Centre (clinic in the community) where a nurse examined her. Based on the examination and disclosure, a decision was made to fly Jessica to Iqaluit, Nunavut, for additional medical attention and support. Iqaluit has the only hospital in the region. Prior to leaving, Child Protection became involved, in addition to the Royal Canadian Mounted Police (RCMP) being notified of the disclosure.
Jessica and her mother had two hours to get ready before the plane came. Tapisa ran home to get a couple of personal items for her daughter before the arrival of the medevac (emergency medical flight). Typically, Jessica would have been placed on a regularly scheduled flight, but she had already missed the flight for that day and the next one was not scheduled for another two days. Based on the time sensitivity of examining Jessica and collecting evidence, a decision was made to travel by medevac. Jessica’s siblings had to stay with extended family in the home while Tapisa and Jessica were away in Iqaluit. We encourage you to keep this case study in mind when reviewing the next section on Inuit history.
Inuit History
Many Inuit reside in small communities in four northern regions of Canada (Inuit Nunangat) including: Inuvialuit (NWT); Nunatsiavut (Newfoundland and Labrador); Nunavik (Quebec); and Nunavut. About 80 percent of Inuit reside across 51 communities within Nunangat (Inuit Tapiriit Kanatami, 2011). Inuit Nunangat encompasses about 35 percent of Canada’s landmass and 50 percent of its coastline (Inuit Tapiriit Kanatami, 2011). According to Inuit Tapiriit Kanatami, it is reported that about 60 percent of Inuit report speaking Inuktut (the Inuit language), and 76 percent of Inuit in Nunavut have Inuktitut as their mother tongue (Government of Canada, 2017). The focus of our chapter will primarily be Nunavummiut (Inuit residing in Nunavut) residing in the Qikiqtaaluq region of Nunavut. The Qikiqtaaluq region consists of 13 fly-in communities.
Pre-Colonialism with Qallunaat (Non-Inuit, Particularly of European Descent)
Consistent with all Indigenous groups at the time, Inuit had a thriving, holistic society and actively met their needs through economic, social organization, and spiritual connections. The economic connections centred on the power of Inuit to meet basic needs of food, shelter and clothing (Arctic Children and Youth Foundation [ACYF], 2018). Within traditional Inuit society and harsh climates, Inuit sustained themselves in their diet by hunting, harvesting and eating all of the animal—this provided a significant source of nutrients and needed sustenance. According to Inuit Tapiriit Kanatami (2011), social organization related to how Inuit organized their relationships with each other (e.g. gender roles, communication protocols, education, leadership, governance, dealing with wrongdoers, etc.) and it was intentional and practiced. The social organization allowed Inuit to have control and agency in day-to-day life. Spiritual practices revolved around the way that Inuit explained their existence through ideas of higher powers, rules of life, relationship with the natural world, and individuals acting as intermediaries with the spiritual world. There are several key historical events that greatly impacted upon the lives of Inuit, primarily colonialism.
1800s-Early 1900s
Whalers began to come to the area from England, Scotland and the United States, as products such as whale bones for corsets, and whale oil were in high demand (ACYF, 2018). Unlike explorers who were just passing through, whalers visited yearly and therefore had a bigger impact on the life of Inuit. According to the Qikiqtani Inuit Association (2013), whalers drew on Inuit knowledge; they employed, traded with, and socialized with Inuit. The relationship between whalers and Inuit introduced regular trade for things like flour, tobacco, textiles, and other metal tools; music such as square dancing (which Inuit still practice today); and social relationships, including babies born from unions between whalers and Inuit (Qikiqtani Inuit Association, 2013).
The first Hudson Bay Company (HBC) trading post was established in Kimmirut in 1912. This expanded to 100 trading posts in the North West Territories (NWT), although not all were HBC. Due to the influence of the trading posts, Inuit started hunting for trade, not just for food, and people grew more dependent on trade goods such as flour and tobacco. This shift caused families to become more individualistic throughout the North, and is seen as the beginning of the use of “money” for Inuit populations (ACYF, 2018). Inuit became dependent, then, on both money and goods, and when these were in low supply, they turned to government services for support.
Canadian Government and RCMP Impact on Inuit
The Royal Canadian Mounted Police (RCMP) initially came to the north in response to threats to Canadian Arctic sovereignty (American and European traders) in the early 1900s. RCMP began travelling to northern communities to enforce Canadian law. In traditional Inuit society, a system was already in place to deal with individuals who were out of line within the group: those who were troublemakers or who caused threats to others (Karetak, 2013). At that time, decisions would be made by Elders, hunters or the whole camp, for the betterment of the camp, and for the good of the group as a whole. This traditional justice worked for the unique lifestyles of Inuit. Increased confusion was created for Inuit with the involvement of RCMP and the new and unfamiliar ways of the Canadian justice system.
Relocation
At the time of the Cold War, many countries fought for sovereignty to claim the North, and Canada sent the military to the North to claim the land. The federal government moved, through forced relocation, the “Canadian Indians” (Inuit) further north in order to claim that land (Inuit Tapiriit Kanatami, 2004; Inuit Tapiriit Kanatami, 2011). At first, Inuit that moved from the Qikiqtaaluk region to higher latitudes (Grise Fiord) understood that they could return to their home communities if they chose. However, this return did not happen. Other relocations occurred with Inuit from northern Quebec, and many suffered greatly and/or died. Extreme weather, and distinct hunting patterns in the unfamiliar territory was the cause. The relocations created artificial settlements, which then turned into communities. On August 18, 2010 in Inukjuak, Nunavik, John Duncan, who was the Minister of Indian Affairs and Northern Development at the time, apologized on behalf of the Government of Canada for the relocation of Inuit to the High Arctic (Government of Canada, 2010).
Figure 1
Apology Statute in Grise Fiord

Tuberculosis in the North 1940s – 1960s
Around 1946, thousands of Inuit across the Canadian North suffered a severe outbreak of tuberculosis (TB). This occurred because of the increase in contact with people from southern Canada and the American military who were stationed in the North. The Canadian government sent a coast guard ship called the C.D. Howe to screen Inuit in the North. Members of the settlements were forced to board the ship and be screened for this and other diseases. However, any individual found to have any signs of TB was not allowed to get off the ship. In this way, children, women, and men of all ages were taken away from their families, and many never returned. The majority of Inuit did not speak English, and the southerners did not speak Inuktut, which affected communication. Inuit would spend an average of two and half years in the hospital due to the tuberculosis outbreak, and during this time, many who had left as children had forgotten their language and crucial survival skills. Most importantly, many individuals had missed out on valuable time with family. Some families to this day do not know the whereabouts of their members who died in TB sanitoriums (Olofsson et al., 2008). As a result, many Inuit lost their traditional connection to land and culture. At one point, one in every seven Inuit were in treatment in the south. By 1970, the long-term hospital treatments slowed the epidemic, but Inuit continue to suffer from TB. On March 8 2019, Prime Minister Justin Trudeau apologized to Inuit for the deliberate mistreatment of Inuit with TB; he committed funding towards travel costs for families who knew where their relatives were buried in addition to funding for marking graves and creating plaques (Government of Canada, 2019).
Residential & Federal Day Schools
Prior to colonialism, Inuit had their own way of educating their children. Because Inuit did not have a writing system, children learned through hands-on experiential learning and oral traditions, including the sharing of legends and stories teaching lessons. Residential schools began in the late 1940s for Inuit, and the children were sent away from their families to attend the schools in places far from their home. If Inuit refused to let their children attend, they would not receive or be eligible for the Federal Family Allowance program—this was the first universal welfare program for families. While attending the school, many children were physically, sexually and mentally abused, could not speak their mother tongue nor were allowed to engage in Inuit practices. The separation of children from their parents during these events severely-affected family attachments, ways of knowing, language, knowledge, communication and the foundation of Inuit kinship society (Healey, 2016). Throughout these atrocities, it was maintained that the schools were present to benefit Aboriginal communities (Macionis & Gerber, 2005). By 1964, 75 percent of Inuit children and youth aged six to 15 were enrolled in the schools (Pauktuutit Inuit Women's Association of Canada, 2007). The children who attended the residential schools lost their identity in many ways. The last residential school in Canada closed in 1996; however, the intergenerational trauma from attending residential school continues today. In 2008, then-Prime Minister Stephen Harper apologized to the victims of residential schools on behalf of the Canadian Government (Government of Canada, 2008).
Dog Slaughter
Dogs played an important role for survival for Inuit (i.e. hunting, travel and protection). In the 1950s and 1960s, it is estimated that 20,000 sled dogs were killed (Qikiqtani Inuit Association, 2013). The slaughter happened all across the Arctic yet was not known as a common occurrence because communities were spread apart, and communication was limited. An Inuit family coming into a town might have had their dog team slaughtered in order to force them to stay in the community. Elders have mentioned that this slaughter could also have been orchestrated to assist the Hudson Bay company (HBC) to sell their skidoos (Qikiqtani Inuit Association, 2013). Eventually, the skidoos replaced sled dogs, and Inuit started living in the communities rather than in small outpost camps. Traditionally, family groups would move to where the hunting was plentiful, but being forced to stay in one area meant that hunting was often less plentiful. Distrust towards the RCMP also began to emerge during this period. On August 14, 2019, then Minister of Crown-Indigenous Relations and Northern Affairs, Carolyn Bennett, apologized on behalf of the government of Canada for colonial practices imposed on Inuit, including sled dog killings—as well as the forced relocations and family separations—to the Qikiqtani Inuit (an Inuit organization representing the Qikiqtaaluk region) (Government of Canada, 2021).
Figure 2
Training Dog Team in Iqaluit, Nunavut

1970s to the Formation of Nunavut
Over the past century, Inuit have been attempting to regain their culture and identity through the work and advocacy of a multitude of local and national level organizations. The organization towards self-government is one example, and organizations that led that process included: 1971 Indian Brother of the NWT; 1971 Inuit Tapirisat of Canada (currently Inuit Tapariit Kanatami); 1972 Inuit Cultural Institute established; and 1981 Inuit Broadcasting Corporation. At present, Inuit Tapariit Kanatami is recognized as the national voice for Inuit of Canada. The role of Inuit Tapiriit Kanatami since its inception has been to support and advance Inuit right to self-determination and self-governance. Through coordination of Inuit Tapiriit Kanatami and its national committees, Inuit were able to secure inclusion of section 35 into the Canadian Constitution Act of 1982, which affirms First Nation, Metis and Inuit rights (Inuit Tapiriit Kanatami, 2004). Inuit Tapariit Kanatami represents four Inuit land claims organizations in Inuit Nunangat and include: Inuvialuit Regional Corporation, Makivvik Corporation, Nunavut Tunngavik Incorporated, and the Nunatsiavut Government.
The Nunavut Land Claims Agreement (NLCA) is a landmark agreement with the federal government, which divided the NWT and created a new territory called “Nunavut.” Nunavut has 28 communities that cover 20 percent of Canada’s landmass and three time zones. Nunavut is separated into three regions (Kitikmeot, Kivaliq and Qikiqtaaluk). It came into being on April 1, 1999. The Legislature began with 19 Members of the Legislative Assembly (MLAs). The government is a consensus government, working for agreement among all its members and respecting Inuit Qaujimajatuqangit (IQ) values (Government of Nunavut, 2007).
The incorporation of Inuit Qaujimajatuqangit (IQ) values into every aspect of modern-day practices within Nunavut exists to maintain and enrich the cultural heritage of Inuit. IQ values are therefore central to Inuit way of living and self-determination. The following IQ values are not only integral to the way of being in Nunavut but also encompass service provisions provision and the delivery.
Inuit Qaujimajatuqangit (IQ values)
- Inuuqatigiitsiarniq: Respecting others, relationships, and caring for people:
- Tunnaganariq: Fostering good spirits by being open, welcoming, and inclusive:
- Pijitsirniq: Serving and providing for family and/or community
- Aajiiqatigiinniq: Decision making through discussion and consensus
- Pilimmaksarniq/Pijariuqsarniq: Development of skills through observation, mentoring, practice, and effort
- Piliriqatigiinniq/Ikajuqtigiinniq: Working together for a common cause.
- Qanuqtuurniq: Being innovative and resourceful (i.e. in solving problems)
- Avatittinnik Kamatsiarniq: Respect and care for the land, animals and the environment
(Government of Nunavut, 2007)
The incorporation of IQ values into service mandates and programming is helping shift the way systems respond in supporting individuals and families within Nunavut. The complex history of Inuit reviewed in the previous section of this chapter has resulted in the impact of intergenerational trauma. Intergenerational or historical trauma refers to trauma experienced by past generations that continues to have an impact on descendants (Crawford, 2013). In many Indigenous communities, such as Nunavut, the presence and impact of intergenerational trauma is commonplace. In recognizing this intergenerational trauma, several initiatives and groups have been working towards a model of service delivery to the most vulnerable segments of the population. The incorporation of IQ values is central to providing appropriate provision of care, as it recognizes the importance of Inuit principles in addressing historical harm. As we transition to our case study, it is important to be mindful of the themes and concepts learned in the previous sections. The application of the previous learning will aid in our perspective with respect to providing care and support to the fictional young Jessica and her family.
Community Response to Care
In this section of the chapter, we will describe the local approach and support given to children and families like those identified in the case study. In the previous section we learned of the history of Inuit through colonialism and the role of national organizations in elevating Inuit voices. Furthermore, the introduction and incorporation of IQ values into programs and services is gradually changing the relationships that community members have to these services. For example, the initial contact for Jessica, following her disclosure, is important as her connection would not have been possible without services explicitly embracing IQ values. Rooted in IQ values is the Surusinut Ikajuqtigiit protocol. The application of this protocol in Nunavut has been able to shift how service providers support the most vulnerable children and adolescents in the community.
Surusinut Ikajuqtigiit (A Group Helping Children)
Based on generations of mistrust from governmental services and entities, forming meaningful relationships is crucial in remote communities such as Nunavut. Traditionally, the basis of strong relationships in Inuit culture has typically related to connection to family, friends and community with a level of equity. The sustained resilience of many Inuit can be attributed to horizontal ties, by which individuals have equal membership and there is reciprocity and cooperation. Vertical ties are relationships in which a member has greater standing with respect to authority, knowledge and wisdom (Brown, 2020). Increasingly, as southerners and governments use vertical ties in their relationship to Nunavut, the sense of belonging and acceptance for Nunavummiut becomes revoked. Vertical ties can be instrumental in some aspects of social work practice; however, when the power balance misaligns, it can become detrimental to the culture, values, and rhythm of the community. Therefore, any collaboration must adhere to traditional community principles as a priority, and must be both reflective and reflexive of generational harm inflicted on individuals and communities by southerners. As social workers, we need to be mindful of the distinction between horizontal and vertical ties. An equitable relationship at the horizontal level can eventually inform the expertise that may be sought at the vertical level.
The creation of Surusinut Ikajuqtigiit (SI) policy as led by governmental departments in Nunavut, is based on the eight IQ values identified earlier in this chapter. Surusinut Ikajuqtigiit recognizes the importance of collaboration (Piliriqatigiinniq—working together for a common cause) within the care provided to the most vulnerable populations. The policy was achieved through active collaboration with governmental organizations who are normally responsible for the care, safety, and education of children and adolescents. The collaboration between these governmental departments, non-governmental organizations, and Elders responding to the needs of the child/adolescent and family is the foundation of SI by protecting children and ensuring that their voices are heard. SI emphasizes the need for multi-disciplinary approaches, collaborative and responsive practices, promotion of child-centred and strength-based investigations, and support services to children and youth. Without the collaboration of community members and important policies as laid out in SI, the creation of coordinated services such as Child Advocacy Centres would not exist (Government of Nunavut, 2020).
The incorporation of SI and IQ values are examples of appropriate connection between horizontal and vertical ties. If there had not been significant engagement and relationship building at the horizontal level, it would be very difficult for the community to have embraced other systems. Similarly, the creation and success of Child Advocacy Centres (CACs) is attributed to an appreciation of ties. Without one service provider willing to acknowledge their limitations to another organization with mutual interests, services would be fragmented, and would not take into account the best interest of an individual or community.
Child and Youth Advocacy Centres
Child Advocacy Centres (CACs) or Child and Youth Advocacy Centres (CYACs) exist in support of children and youth who have experienced different forms of abuse/maltreatment (Hickey, 2015). CACs/CYACs provide child-centred environments for the person receiving support. Although the CAC model may have variations across regions, it is recognized as an overall best practice model of care for response to child/adolescent abuse (Bertrand et al., 2018). The Centres are created out of a need to improve disjointed service collaboration and lack of child-centred processes, which inevitably causes more trauma to a child after abuse/maltreatment. As highlighted in Table 1, CAC/CYACs have been shown to have many short- and long-term benefits (Bertrand et. al., 2018; Herbert & Bromfield, 2016).
Table 1
Benefits of CACs
| Short Term Benefits | Long Term Benefits |
|
|
Note. Adapted from Herbert and Bromfield, 2016.
CACs in Nunavut
It is reported that child abuse and maltreatment rates in Nunavut are approximately 10 times that of the national average (Representative of Children and Youth, 2019). The stark difference in these rates has resulted in a demonstrated need for improved service coordination in Nunavut to support children and adolescents. Based on a community needs assessment, it was determined that a CAC would provide supports using a child-centered, culturally-relevant response to young Nunavummiut (people residing within Nunavut) who have experienced child abuse and neglect (Qaujigiartiit Health Research Centre, 2010). The embracing of a CAC in Nunavut was encouraged through service partners in the creation of the SI.
With the non-governmental organization (NGO) Arctic Children and Youth Foundation (ACYF) as lead, the following organizations and departments were involved in the collaboration: Justice, Health, Education, Child and Family Services, the RCMP, and Nunavut Tunngavik Incorporated (NTI). These organizations signed a memorandum of understanding (MOU). An MOU is an agreement between distinct parties with mutually-accepted expectations. The expectation was the commitment of the highlighted parties to create a CAC in Nunavut where children and their families can feel safe and comfortable to access support.
The Umingmak Centre became operational in 2019 in Iqaluit, Nunavut. Since opening, the Umingmak Centre has provided services and resources to children and families where there have been disclosures or suspicions of crime relating to abuse (i.e. exposure to significant caregiver violence, death and homicide, sexual abuse, neglect and physical abuse). The Centre uses best practice in child abuse investigations, assessment, support and treatment by coordinating with its service partners (e.g. RCMP, Child and Family Services, Pediatricians, Justice, Education and allied community members).
Umingmak is the Inuktitut word for muskox. Umingmaks are known to be very protective of their young. When a young umingmak is in danger, the adults create a protective barrier around them to shield them from harm. The analogy of protection is rooted in the purpose of the centre and community values around caring for vulnerable children and adolescents.
Figure 3
Umingmak Centre
The Umingmak Centre has highly skilled professionals who provide quality service through a trauma informed lens with children/adolescents and their families.
Roles at the Centre
To help describe how a CAC works, and how it might serve the needs of someone like Jessica in our case study, we will describe the role of each member of the team at the CAC.
Child/Adolescent Advocates at the Umingmak Centre are responsible for supporting children/adolescents, and their non-offending caregivers with age specific trauma informed support. Advocates are the main point of contact for children and non-offending caregivers. They are ultimate service and system navigators following the completion of the interview or investigative process and are a source of psychoeducation to families and children/adolescents.
The role of the Trauma and Inuit-trained Counsellors at the Centre is to support families, children/adolescents through trauma-informed information and supports. Counselling can occur in the context of individual, family and group formats. Given the disruptive nature of trauma in a family setting, family therapy allows individuals to incorporate the various available resources. With cultural and individual family considerations, family therapy can include whoever the child/adolescent views as a supportive person. Counselling can be tailored to individual needs.
The Umingmak Centre works closely with local Pediatricians. The role of the pediatrician is to provide clinical support in the investigative process, and to complete a forensic examination (collect DNA samples from child/adolescent for testing and provide essential medical care). Pediatricians also provide reassurance examination for cases where there has been a historical disclosure (disclosure that occurred outside clinical limits for examination). They also meet with the child/adolescent and their non-offending caregiver as needed in order to provide follow-up care. The Centre works closely with specially trained RCMP Interviewers in child/adolescent cases of maltreatment called the Specialized Investigation Team (SIT). The SIT was formed in 2019 as part of the Nunavut RCMP V Division. The SIT is focused on assisting and conducting investigation of sexual crimes involving children and adolescents across the territory of Nunavut. The officers will typically conduct their interview in plain civilian clothing to reduce stress and intimidation possibly triggered by the uniform. For many children/adolescents who have been interviewed at the Centre, it is typically the first time seeing an officer in civilian clothing. The interviewer’s role is to acquire as much information relating to the disclosure as possible in order to determine if a charge can be made.
The role of the Child Protection Worker is essential to the investigative process of the particular allegation/charge, and ongoing after that time as needed, to ensure the safety of the child/adolescent. Protection Workers are also known as Social Workers within Nunavut. A Protection Worker will typically bring the family to the Centre, observe the interview for further interventions and as support to the family. Simultaneously observing the interview eliminates the need for further interviews which might be distressing or retraumatizing.
Case Study and Multidisciplinary Care
Now that we have reviewed the history of Inuit in Nunavut and the CAC model, we can look at how this multidisciplinary care would look for Jessica from our case study. We will review the steps and process of investigation typically followed in Nunavut, as well as the start of healing for Jessica and her family. We learned earlier that the creation of the Surusinut Ikajuqtigiit (SI) policy was to encourage collaboration following disclosures of abuse. Disclosures of childhood sexual abuse within Nunavut typically are received through Child Protection Services and the RCMP. As part of the SI, there is an emphasis on the importance of community partners ensuring that their efforts to protect children from abuse are integrated, effective, and culturally appropriate.
Each of the smaller communities in Nunavut has a Community Health Centre (CHC). Community Health Centres provide a variety of health services (i.e. emergency, pre-and post-natal, immunizations, public health, counselling, mental health and etc.) and are typically supported by community members and nurses. In the Qikiqtaaluk region, physicians typically fly into the community on a rotational basis every few weeks. Nursing staff connect with physicians via phone or email (depending on urgency) to best support clients locally. For more complicated or urgent cases, the individual is flown to Iqaluit via scheduled flights or medevac (air ambulance).
In this fictitious case of Jessica, her disclosure activated different reporting agencies within her community of Kinngait. Upon being examined by the Community Health Nurse (CHN) at the Health Centre, the CHN had to contact Child Protection Services as part of her Duty to Report, as well as the RCMP. As we have previously learned, Child Protection is responsible for the safety of the child/adolescent and will determine if the child needs protection, whereas the RCMP investigates to determine if criminal charges are to be laid.
Due to the time sensitivity in the case of Jessica, the CHN sought direction from the physician who was on call in Iqaluit. Based on the physician consultation, the decision was made to have Jessica flown to Iqaluit for further care. A full investigation was not possible in the community due to the timing of the scheduled plane arrival, so both Child Protection Services and the RCMP made sure to connect with counterparts in Iqaluit.
Jessica Arrives in Iqaluit
In the case study focusing on Jessica, arrangements were made with Child Protection Services to provide the family with transportation at the airport. As the flight arrived late, the Child Protection Worker ensured that the family was taken to the local medical hotel/boarding home for individuals and families visiting Iqaluit for medical care. Arrangements were subsequently made with Jessica and her mother to be picked up in the morning to come to the Umingmak Centre.
Upon arriving at the Umingmak Centre, Jessica and her mother Tapisa were welcomed by the Advocate who is Inuk (singular for Inuit). At the onset of the therapeutic relationship, the Advocate typically provides a tour of the Centre to the child/adolescent and their non-offending caregiver, as was the case for Jessica and Tapisa. The Advocate reinforces the existing supports and highlights that the Centre is dedicated in building community relationships and resources to help families throughout the journey from disclosure to healing.
Often country food (food that is local to Inuit) and beverages are offered and shared during this time, which is consistent with Inuit culture. The experience can at times be quite overwhelming for non-offending caregivers as many caregivers are flooded with emotions about their own past traumatic experiences. As we learned earlier in this chapter, the impact of intergenerational trauma is pervasive within northern communities. Being in supportive spaces like the Centre can at times result in many caregivers disclosing their own experience of abuse (typically sexual maltreatment) during the introduction meeting with their child/adolescent. Caregivers of children/youth involved with the Umingmak centre have been universally thankful for the existence of services through the Centre for their child/adolescent, but often talk about the contrast in the potential impact that the Centre’s existence would have had within their own adult lives and healing had it existed for them during their childhood. As needed, the Centre typically connect caregivers to an Inuit Trained Trauma Counsellor.
Specialized Investigative Team (SIT)
Jessica was introduced to two female members of the RCMP SIT who conducted her interview. Typically, one will lead the interview and the other will monitor the interview in another room along with the Child Protection Worker. Jessica is bilingual (fluent in Inuktitut and English), but preferred to be interviewed in English, and therefore was interviewed by an English-speaking interviewer. In the event that Jessica was unilingual in Inuktitut, an RCMP member fluent in Inuktitut would have taken the lead on the interview, or an interpreter would have been provided. In Nunavut, there have been significant recognition for the need to train additional RCMP officers who are fluent in Inuktut.
Medical Examination
Jessica was then introduced to the pediatrician. The pediatrician spent time with Jessica and her mother prior to the exam, to allow them to feel comfortable and ask questions. The clinic room is child friendly and is similar to any other clinical exam room in a community health centre or hospital setting. The pediatrician provided a medical assessment, which in this case included a forensic examination and obtaining forensic evidence with a sexual assault evidence kit (SAEK). The specifics around evidence collection were provided by the forensic interview that was completed. With consent, Jessica’s mother was present for the entire examination.
Case Review
Following the interview with Jessica, the SIT members met with the pediatrician to review their respective interviews and assessments. In this case, there were significant findings by the pediatrician during the examination. It was also helpful that Tapisa kept Jessica’s clothing from the sexual assault which was then sent out for testing. The majority of sexual assault evidence collection is sent to Manitoba to the RCMP national forensic lab for testing. During this review, the SIT lead investigator also confirmed that Jessica gave a disclosure, which resulted in her uncle being arrested and charged.
Following this discussion, the SIT members, pediatrician and advocate met with Tapisa and Jessica to inform them about next steps. Tapisa became emotional after learning about the disclosure and medical findings. Tapisa expressed worries about being evicted from the familial home as it is owned by her brother (the alleged perpetrator). The team offered reassurance that the support received by Jessica would be a big factor in determining the positive healing journey ahead for her. Victims of sexual abuse have better treatment outcomes if they feel believed by the person they disclose to (Humphreys, 1992; Vaplon, 2015). Tapisa was offered additional support through the Inuk Trained Counsellor and also met with the Child Protection Worker to develop a safety plan.
At this point, an exploration of a treatment plan was reviewed with the multidisciplinary team at the Centre. Typically, for cases within the Qikiqtaaluk region, interdepartmental collaboration occurs and families are supported to travel and have ongoing support in their home community (i.e. Mental Health Nurse, Outreach Worker, Wellness Counsellor and in some cases an Elder).
In the case of Jessica, following the immediate arrest of the uncle, Tapisa, Jessica and their family were evicted from the home. This created an emergency situation of homelessness. According to Inuit Tapiriit Kanatami (2014), about 39 per cent of Inuit in Inuit Nunangat live in overcrowded homes compared to four percent of all Canadians. The significant disparity can create additional stressors and pressures for families fleeing violence. In the case of Jessica, the Protection Worker was able to make arrangements to have Tapisa and her children brought to Iqaluit for emergency housing. Nunavut operates family violence shelters in each of the three regions.
Healing Considerations
The deleterious long-term impact of child maltreatment and trauma for children/adolescents often manifests in the breakdown of family systems and poor psychosocial outcomes (Buss et al., 2015). Within treatment, the goal is recovery for the individual, family and caregivers. At the Umingmak Centre, individual trauma counselling is available for children and youth who meet criteria for counselling along with their non-offending caregivers. The treatment program provides principles of trauma-informed practice which emphasizes: trust, safety, choice and control. The goals of the programs are to reduce the negative impacts of abuse, trauma, and maltreatment while fostering resilience. Each client’s treatment plan is created collaboratively with the client and the multidisciplinary team, as the ultimate goal is to allow the child to heal holistically in the domain of the physical, developmental, cultural and spiritual self.
Being believed by a non-offending caregiver, following disclosure of abuse, can at times be transformational for the child/adolescent providing the disclosure (Bolen & Lamb, 2004; Humphreys, 1992). Simply, within the therapeutic process, non-offending caregivers possess the ability to play an essential role in supporting their child/adolescent through traumatic disclosures and subsequently the experience itself. In keeping with the importance of familial relationships among Inuit, there is active mobilization of the child’s support systems. The additional recognition of the non-offending caregivers highlighting their own historical and sometimes active traumas, can at times complicate the healing journey for the family, particularly the child/adolescent (Manion et al., 1996). The complexities of supporting the family system through a culturally-centric approach in helping members of the family heal in their recovery journey, specifically focusing on the challenges facing the non-offending caregivers and their respective traumas, is quite significant. The role of the Inuit Trained Trauma Counsellors assists in making this work successful.
Multidisciplinary teams can be incredibly helpful for families such as Jessica’s in navigating their healing journey through the linking of services and resources available within the community. Although, discussion and actions coming from these teams’ meetings will look different for every child/family, the collaboration of partners remains essential in better understanding and meeting the needs of each child.
The well-being of children is impossible to separate from the well-being of their caregivers and others within their community (McKenzie et al., 1995). Within the literature it is well understood that non-offending caregiver support typically has four major dimensions: believing the child, protecting the child, emotionally supporting the child, and obtaining resources for the child (Priebe & Göran, 2008). The shame associated with sexual abuse is at times amplified in remote communities such as Nunavut. As the child/adolescent moves through their trauma healing, the objective is to create new narratives which will empower them to reconnect with previous joys and normalcy within their lives and community. Part of this reconnection centres around family and strengthening the bond associated with same. In collaboration with the family, the Centre is actively finding ways of incorporating traditional healing (i.e. on the land programming) to increase the reconnection for the child/adolescent. Additionally, part of the healing includes increasing the child/adolescent’s cultural identity through mentorship with the Inuit Advocates at the Centre. For Jessica this includes learning about her own Inuit history through the experience of running a dog team or being part of therapeutic groups with peers who have had similar experiences.
Figure 4
Being on the Land

Levels of Social Work Practice in Nunavut
Now that we have described a case scenario, we will dissect the levels of social work practices in Nunavut, while keeping this case in mind.
At the micro level, it is important to recognize some of the barriers that individuals and families have to services. Clients like Jessica and her family received a variety of supports including individual, family and group therapy that was individualized to their specific needs. Within this work, clients are actively referred to other services within the community in order to achieve their full potential and healing needs. The involvement or exclusion of families within the therapeutic relationship at the micro level can also instill or breakdown further issues at this level. Being a social worker within a remote community such as Iqaluit is more than simply providing service and linking people to services. The role and responsibility has many important considerations, especially when working with vulnerable populations. Social workers need to be mindful of the generations of harm and the perpetual continuation of this within systems. More importantly the level of power and trust at the micro level needs to be respected and recognized when navigating larger systems with families.
As social workers, our work with clients at the mezzo practice level typically involves participation in working groups and advocacy towards achieving equitable services within the community. An example of this includes the formation of the Arctic Child and Youth Foundation (ACYF), which was founded by community leaders such as the current Governor General of Canada, Mary Simon. In 2003, along with other community members, Mary Simon created the organization ACYF to support children and youth of Nunavut to navigate their quickly changing world from the traditional Inuit way of life. About a decade later, the prevalence of childhood sexual abuse was becoming even more apparent, and leading community members created a working group to address this important issue. The first Child Advocacy Centre (CAC) in Nunavut is an example of the gradual grassroots movements to address community issues at the mezzo level. Families, like Jessica’s, are able to receive coordinated services as a result of organization at the mezzo level.
Similar to the working group in the mezzo system, it took a couple of community leaders to focus on changes at the macro practice level. As a result of their efforts over the past two decades, changes have occurred at the political level by having a Memorandum of Understanding (MOU) created within all the departments in Nunavut who are responsible for the well-being of children, such as Education, Health, Justice, Child and Family Services, the RCMP, and Nunavut Tunngavik Incorporated (NTI). The support of leaders from these departments for this MOU has allowed the opportunity for there to be a focus on children and adolescents in Nunavut to receive the coordinated, consistent care they deserve with respect to adverse experiences such as abuse and maltreatment. The opening and subsequent success of the Umingmak Centre has also encouraged governmental and non-governmental funders to create a second CAC within the Kitikmeot region of Nunavut.
Without the advocacy of social workers, allied professionals and community members doing individual and family interventions and then shinning a light to the important and prevalent issue of child abuse, there would have been no working groups, political will and data collection to support the need of a transformative approach to addressing child abuse in Nunavut. The collaboration of these leaders would not have been possible without the ability to contextualize the issue of abuse and the manifestation of it as evidenced by significant harm inflicted on the community following colonization. Community members actively recognized the impact of the historical harm and transformed it through an adherence to Inuit Qaujimajatuqangit (IQ) values, working collaboratively across sectors for the betterment and future of the most vulnerable populations.
Ethical Considerations for Working in the North
The urban metaphor of being neutral and understanding of a culture does not capture the knowledge and history that must be acquired prior to working within a northern community setting such as Nunavut. There is a strong foundation of culture and experience in each community that requires respect from southern workers. Without the provisions outlined in social work codes of ethics, the manner in which professionals conduct themselves could adversely affect not only the worker but the type of work done with vulnerable clients and their families. An adherence to regulated bodies such as a college of social work, can ensure that the work is being guided with the best interests of our clients, especially in marginalized and vulnerable communities in Nunavut. In stating this, our clients are left at a disadvantage when we engage in the work without any accountability through connection with a regulated body. Currently, in Nunavut, there is no mandate to be part of a college of social workers, which can lead to concerns especially when the individual is a new graduate. Ideally, a competent social worker is guided by legislation so that they are better able to work within those parameters or possibly challenge policies. When practitioners do not have a professional college to belong to, this can create issues with appropriate checks and balances, which can leave the client in a situation with limited recourse if ethical violations occur. In remote communities such as Nunavut, having a professional college affiliation is essential when considering the history of harm.
Although professional membership is not mandatory, many social work practitioners in Nunavut have opted to be part of the Association of Social Workers in Northern Canada (ASWNC). The ASWNC represents social workers in the Yukon, Northwest Territories and Nunavut. The aim of the Association is to provide support to social workers through professional development and representation at the territorial and national level. The values in the Code of Ethics adhered to by ASWNC follows that of the Canadian Association of Social Workers (2005), which includes: respect for the inherent dignity and worth of persons; pursuit of social justice; service to humanity; integrity in professional practice; confidentiality in professional practice; and competence in professional practice.
The issues that arise in northern social work practice include practicing beyond our competence, dual relationships, having too much access to information, and limited supervision. An additional issue is professional drift which can occur in northern communities where a social worker can abandon the purpose associated with the profession in place of roles associated with other disciplines. The role of a regulatory body would be to ameliorate the emergence of such issues by keeping social workers within the boundaries of their profession. Although there is no regulatory body within Nunavut, practitioners are still morally obliged to uphold these standards and adhere to these boundaries through membership involvement and appropriate supervision. When practicing in northern and remote communities, the lack of resources or “experts” within communities can result in many social workers engaging in work that is normally outside their expertise, or a practicing social worker might align oneself with the practice of other professionals within the community (Schmidt, 2009). For instance, a social worker might be asked to assist with a role outside their usual scope, simply due to a shortage of staff. Although well intentioned, this alignment may lead to service and care that is not client centred. Social workers who embrace these additional roles for the sake of resource scarcity also risk denying clients their right to feel empowered. Due to the nature of social work practice in the north, we are also privy to more details of our clients’ personal lives, as we are neighbours with our clients; we see them at the grocery store and at the hockey rink. This familiarity is not the case in other geographical settings. Truly, the combination of these factors places us in various ethical predicaments.
For social workers in northern practice, appropriate supervision is essential in ensuring that the described challenges are avoided. In balancing a client’s right to self-determination along with an ethical dilemma, the role of a culturally-diverse multidisciplinary team is even more important in all decision-making processes.
As social workers, our professional knowledge, insight and experience allow clients to work with us and hopefully trust us. If barriers exist to us upholding that professionalism, this may impact our ability and growth as a social worker, which in turn will negatively impact clients. Any regulatory body for our professional code of ethics is a reference point that allows us to do the work that we are intended to do within this helping profession. Furthermore, our removal from this process, or lack of acknowledgement of the historical context, would be harmful not only to our therapeutic relationships but also to the growth experienced by our clients.
Challenges and Barriers
Geography poses the most significant barrier to families and their ability to access professionals, including social workers. Finances for physical travel are obvious, but the latent barriers geography poses for families are perhaps more dangerous to meaningful access. The implications of Jessica and her caregiver travelling some distance for care outside her home community are significant. Without access to childcare, families with a child/adolescent in need of medical practitioner care, as well as care from allied professionals (including social workers) at a Child Advocacy Centre (CAC) may be forced to choose between accompanying the child to the CAC and leaving remaining children in non-ideal child care arrangements or in the temporary care of a child welfare agency. In addition to child care issues, accessing care may mean parents are forced to choose between taking unpaid leave from work and forgoing wages needed to feed and house their families. As social workers in remote communities, we need to be aware of these realities, as they provide essential context to any client intervention and goal setting. Awareness of these realities also ensures that we manage our expectations of our clients by not asking too much of them.
The reality of the case of Jessica highlights many inequities that continue to exist for victims of child abuse and family violence. Limited availability of resources typically means that the victim has to relocate in order to access support. In some instances, the abuse is maintained and perpetrated as the victim(s) are unable to leave, and there are no emergency resources within the community. The daunting reality faced by families like Jessica’s present additional stressors and systemic barriers for families in their healing. In this situation, following the disclosure, Jessica had to travel out of her home community for additional care and supports. Jessica also learned that, as a result of her disclosure, she and her mother were no longer welcomed in the familial home. As the family considered these new changes, Jessica and her siblings also had to consider changes to their home environment, social life and emotional supports. Tapisa also has to be able to navigate new employment and support systems for herself and her family.
The challenges facing the child/adolescent in a remote community in Canada are evident and need to be acknowledged. Southern social workers in remote communities such as Nunavut need to understand the barriers in place and how these barriers may affect children and families. This understanding will help social workers and allied professionals in connecting and supporting families successfully at the micro/mezzo/macro levels. As seen by the progression of grassroots organizations, no social worker or medical practitioner is going to change the world overnight. Rather, the role is to understand and chip away at the challenges that have been cemented through generations of trauma and wrong-doing. Understanding the community, knowing the families and their challenges, understanding the available resources and the lack of resources facing families, and listening to concerns is crucial to transformational and meaningful change.
In addition to understanding children/adolescents, their families, and the communities from which they come, it is extremely important that social workers from the south operate from the perspective of diligently making connections and knowing what resources are locally available. Whether it is the Community Health Nurse (CHN), the Child Protection Worker, a community justice worker, a government representative, or an Elder, such individuals will understand family dynamics, relationships, and any existing trauma far more than someone operating from a stand-alone place of “expertise.”
Conclusion
Inuit have lived in the Arctic region for over 5000 years and are the original inhabitants (Inuit Tapiriit Kanatami, 2004). Prior to colonization, Inuit resided in small, family-based camps, and were nomadic, travelling seasonally on the land for hunting, fishing and gathering all their food and resources. To survive the harsh climate, Inuit typically depended on each other to meet their basic physical needs (i.e. food and shelter). Established values sustained families throughout these hardships, and the resilience of Inuit has sustained them over the years. The role of Inuit Qaujimajatuqangit (IQ) values have also been instrumental in the maintenance of culture and identity. Furthermore, the incorporation of IQ values in policies and organizations has proved beneficial in the lives of Inuit, but this is an active process and practice, especially for southerners working in Nunavut with children/adolescents and their respective families.
As professionals working in remote communities such as Nunavut, it is our duty to be informed about the histories and oppressions experienced by our clients. The deleterious long-term impact of child maltreatment and trauma for children/adolescents often manifests in the breakdown of family systems and poor psychosocial outcomes (Buss et al., 2015). The discovery of a child experiencing severe maltreatment can cause trauma to each family member, and can have serious implications for the lives of all family members. How a parent responds to a child disclosing abuse can also have a dramatic influence on the child. In a territory such as Nunavut, with a well-documented history of intergenerational trauma, social and physical inequalities, the impact of a disclosure in the family is typically experienced differently in that the dynamic shift can be significant (Representative for Children and Youth, 2019). Multidisciplinary teams can play a significant role in the healing of families, especially when the team is representative of the uniqueness of the community and its needs.
Based on the two decades of commitment towards the realization of the first CAC in Nunavut, it is easy to appreciate the complexity and challenges of historical harm. The Umingmak Centre plays the vital role of supporting children/adolescents with disclosures of abuse (e.g., sexual, physical, neglect and exposure to violence). The multidisciplinary approach is rooted in recognition of cultural perspectives and understanding of the initial disclosure and healing journey. Based on the uniqueness of the remote community, services available to the children and their respective families are fostered and enriched from a cultural perspective by creating allies within the community along with fostering service partnerships.
In supporting a child/adolescent in their healing, family involvement must be central to the child/adolescent’s overall recovery. Childhood sexual abuse is relational by nature, and therefore the importance of aligning with families to foster further healing through social learning and corrective narratives has the potential to sustain wellness within families. Increased connection and support are key to increased family empowerment, healing, safety, sense of self and resilience, and reduced generational transmission of trauma response.
Activities and Assignments
- If you were to start planning to open a CAC in a northern community close to where you are now, whom would you speak to first, and what would be your priorities in planning? Apply the concepts of micro/mezzo/macro to your answer.
- You are starting a new job in Kugluktuk, Nunavut as a social worker. You have recently graduated and are very keen. What do you expect will be your three biggest challenges, and how might you overcome those challenges?
- As part of your self-care, you have joined an extracurricular activity playing frisbee. One of your teammates is a parent of a family that you are involved with at work. How would you navigate this interaction?
- A caregiver you are supporting informs you that she is worried about a case conference at their child’s school. How would you apply the Surusinut Ikajuqtigiit in this situation to ease her worries about the meeting?
- This chapter highlighted the many challenges experienced by Jessica in leaving her home community to receive service. As the social worker helping the family with their transition to their new community, which IQ values will you apply to guide this process?
References
Arctic Children and Youth Foundation. (2018). Caring for others, caring for ourselves: Trauma awareness for young leaders.
Bertrand, L.D., Paetsch, J.J., Boyd, J.P., & Bala, N. (2018). Evidence supporting national guidelines for Canada’s child advocacy centres. Government of Canada, Department of Justice.
Bolen, R. M., & Lamb, J. L. (2004). Ambivalence of nonoffending guardians after child sexual abuse disclosure. Journal of Interpersonal Violence, 19(2), 185-211.
Brown, G. (2020, July 14). Difference between horizontal and vertical relationships. Difference Between Similar Terms and Objects. http://www.differencebetween.net/business/difference-between-horizontal-and-vertical-analysis/
Buss, K. E., Warren, J. M., & Horton, E. (2015). Trauma and treatment in early childhood: A review of the historical and emerging literature for counselors. The Professional Counselor, 5(2), 225-237.
Canadian Association of Social Workers (2005). Code of ethics. https://www.caswacts.ca/files/attachements/casw_code_of_ethics.pdf
Crawford, A. (2013). The trauma experienced by generations past having an effect in their descendants: Narrative and historical trauma among Inuit in Nunavut, Canada. Transcultural Psychiatry, 51(3).
Government of Canada. (2008, June 11). Statement of apology to former students of Indian Residential schools [press release].
Government of Canada. (2010, September 15). Apology for the Inuit High Arctic relocation [press release].
Government of Canada (2017, Oct 25). Census in Brief: The Aboriginal languages of First Nations people, Métis and Inuit.
Government of Canada. (2019, March 8). Statement of apology on behalf of the Government of Canada to Inuit for the management of the tuberculosis epidemic from the 1940s-1960s [press release].
Government of Canada. (2021, August 12). Minister of Crown-Indigenous Relations delivers apology to Qikiqtani Inuit [press release].
Government of Nunavut. (2007). Inuit Qaujimajatuqangit Education Framework for Nunavut Curriculum. https://www.gov.nu.ca/information/inuit-societal-values
Government of Nunavut. (2020). Surusinut Ikajuqtigiit: Nunavut Child Abuse and Neglect Response Agreement.
Healey, G. (2016). (Re)settlement, displacement, and family separation: Contributors to health inequality in Nunavut. The Northern Review, 42, 75-96.
Herbert, J. L., & Bromfield, L. (2016). Evidence for the efficacy of the child advocacy center model: A systematic review. Trauma, Violence & Abuse, 17 (3), 341–357.
Hickey, S. (2015, July). Child advocacy centres and child and youth advocacy centres in Canada: National operational survey results. Research and Statistics Division, Department of Justice Canada.
Humphreys, C. (1992). Disclosure of child sexual assault: Implications for mothers. Australian Social Work, 45(3), 27-35.
Inuit Tapiriit Kanatami. (2004). 5000 years of Inuit history and heritage. https://www.itk.ca/5000-years-inuit-history-heritage/
Inuit Tapiriit Kanatami. (2011). Inuit regions of Canada.
Inuit Tapiriit Kanatami. (2014). Comprehensive report on the social determinants of Inuit health. https://www.itk.ca/social-determinants-comprehensive-report/
Karetak, J. (2013). Conversations of Inuit elders in relation to the Maligait (Inuit laws). Nunavut, Department of Education.
Macionis, J. J., & Gerber, L. M. (2005). Sociology (5th ed.). Pearson Education Canada Inc.
Manion, I. G., McIntyre, J., Firestone, P., Ligezinska, M., Ensom, R., & Wells, G. (1996). Secondary traumatization in parents following the disclosure of extrafamilial child sexual abuse: Initial effects. Child Abuse and Neglect, 20, 1095–1109.
McKenzie, Seidl, E., & Bone, N. (1995). Child and family service standards in First Nations: An action research project. Child Welfare, LXXIV(3), 633–654.
Olofsson, E., Holton, T., & Partridge, I. (2008). Negotiating identities: Inuit tuberculosis evacuees in the 1940s-1950s. Inuit Studies, 32(2), 127–149.
Pauktuutit Inuit Women’s Association of Canada. (2007). Sivumuapallianiq: National Inuit residential schools healing strategy: The journey forward. Pauktuutit Canada.
Priebe, G., & Göran, C. (2008). Child abuse & neglect child sexual abuse is largely hidden from the adult society: An epidemiological study of adolescents’ disclosures. Child Abuse & Neglect, 32 (12), 1095-1108.
Qaujigiartiit Health Research Centre. (2010). Needs assessment of child and youth mental health services in Nunavut. Qaujigiartiit Health Research Centre.
Qikiqtani Inuit Association. (2013). Qikiqtani Truth Commission final report: Achieving Saimaqatigiingniq. https://www.qtcommission.ca/sites/default/files/public/thematic_reports/thematic_reports_english_final_report.pdf
Representative for Children and Youth. (2019). Our minds matter: A youth-informed review of mental health services for young Nunavummiut. https://rcynu.ca/sites/rcynu.ca/files/RCYO_MHReview_EN.pdf
Schmidt, G. (2009). What is northern social work? In R. Delaney & K. Brownlee (Eds.), Northern and rural social work practice: A Canadian perspective (pp. 1-17). Lakehead University Centre for Northern Studies.
Vaplon, C. S. (2015). The effects of parental response on their children’s trauma experience [Master’s thesis, St. Catherine University]. Sophia.
Consistent with other remote Indigenous communities, social work in Nunavut has many unique challenges and limitations. The current chapter aims to explore and understand approaches to these challenges, through the introduction of a case study highlighting common realities across Nunavut. We will further describe several practice approaches and competencies in navigating the case study. As social workers, we must understand the historical and social complexities of Inuit populations to consider any approach or intervention in the provision of service. It is our hope that the introduction of Inuit history and its context will enrich your approach to care within our region. We introduce and explain the Child Advocacy Centre (CAC) model, which works within the Inuit Qaujimajatuqangit (IQ) principles. We will also explain the Umingmak CAC and how its introduction has changed the response to childhood trauma within our jurisdiction, and allowed for more inter-departmental communication and collaboration. This change has ultimately shifted the response to care of our most vulnerable children and adolescents in our community.
This chapter will review Inuit history, values, community response to supporting children and adolescents with disclosures, as well as challenges, barriers and interventions. Although the content may seem extensive, we recognize that it may still not feel complete in capturing the complexity of social work in Nunavut. As a future social worker, you need to immerse yourself in the content while maintaining a critical lens of the larger impact of colonialism on service provision. The chapter might also illicit certain reactions based on your own social location and your beliefs about how service delivery should look or be implemented. If you find yourself challenged at certain moments, manage the discomfort as you are able and then return to the chapter when you are ready.
Learning Objectives
By the end of this chapter, you will have the opportunity to:
- Understand the historical context of Inuit in the Arctic
- To be introduced to Inuit societal values
- To explore best practices in community response to care
- To describe Child Advocacy Centres, and the first Child Advocacy Centre in Nunavut
- To recognize the importance of working in multidisciplinary teams
- To explore ethical considerations, barriers and challenges in the context of providing social work in Northern Canada
Inuit history from pre-colonialism to current realities will be reviewed. We acknowledge that we are not Inuit and do not represent Inuit. We write about Inuit culture and heritage only to assist in the description of unique social work practice in our location. We encourage you to look to Inuit organizations and individuals for further information on this subject. Our intention is to provide some foundational understanding relating to themes of distrust in service provision caused by colonialism. Inuit societal values will be explored in the context of resilience and the sustaining of Inuit traditions. Inuit societal values are integral to policy enactment and subsequently service provision. The review of values will add another layer of learning about the strength of Inuit. As an emerging social worker, your understanding of a community response to care is integral to service provision. At times, you may feel disconnected from the theory as realities of practice crystalize; you are encouraged to challenge your learning during this process. We will review community response to care in our Inuit community and the complexity of service provision. Child Advocacy Centres (CAC) have been transformative in many communities with respect to service provision for children and adolescents who have disclosed distinct forms of maltreatment. Therefore, we will review the history of CACs and the impact in communities, particularly Nunavut.
A part of Inuit societal values relates to working together for a common good. This value is explored through a discussion about working in multidisciplinary teams. As social workers we are actively confronted with ethical dilemmas, and these can be unique in remote communities such as Nunavut where your neighbour might also be your client. Attention to ethical considerations in small communities will be explored. We will conclude our learning by discussing barriers and challenges experienced by social workers in Nunavut. In particular, the section will highlight some of the progress relating to service delivery but will also review a call to action in highlighting the challenges ahead. Prior to our learning on Inuit history, to provide additional context to social work in Nunavut, please review the case study of Jessica, which will guide this chapter.
Case Study of Jessica
This fictitious case study of Jessica will focus on the realities of remote communities, such as service pathways for those located in Nunavut. The authors aim to highlight specific challenges faced as a result of this context.
Jessica is a 10-year-old Inuk girl who is currently in grade 5 in Kinngait, Nunavut. Jessica has three younger siblings and resides with them and her mother (Tapisa) within a multigenerational household that is owned by her Uncle (Jamesie); there are 11 people residing in the three bedroom home. Tapisa has a history of alcohol dependence but in the past year has focused on her personal healing. The former partner (Peter) of Tapisa died by suicide when Jessica was 5 years old.
A couple of years ago, Tapisa started working as a machine operator for a mining company. Tapisa works in another fly-in community on a three week rotation and then is home for three weeks. During the time Tapisa is away working, Jessica and her siblings are cared for by extended family members within the home.
During a recent outburst in the home by Jessica, Tapisa took her daughter aside to help regulate her. Jessica disclosed to her mother that she was being sexually abused by one of her uncles during the period that Tapisa was working at the mining company. Jessica pointed to pain in her vaginal area. Tapisa was very shocked and emotional with her daughter. Tapisa reassured her daughter that she was safe, thanked her for telling her, and assured her that she would deal with it.
Tapisa took Jessica to the Community Health Centre (clinic in the community) where a nurse examined her. Based on the examination and disclosure, a decision was made to fly Jessica to Iqaluit, Nunavut, for additional medical attention and support. Iqaluit has the only hospital in the region. Prior to leaving, Child Protection became involved, in addition to the Royal Canadian Mounted Police (RCMP) being notified of the disclosure.
Jessica and her mother had two hours to get ready before the plane came. Tapisa ran home to get a couple of personal items for her daughter before the arrival of the medevac (emergency medical flight). Typically, Jessica would have been placed on a regularly scheduled flight, but she had already missed the flight for that day and the next one was not scheduled for another two days. Based on the time sensitivity of examining Jessica and collecting evidence, a decision was made to travel by medevac. Jessica’s siblings had to stay with extended family in the home while Tapisa and Jessica were away in Iqaluit. We encourage you to keep this case study in mind when reviewing the next section on Inuit history.
Inuit History
Many Inuit reside in small communities in four northern regions of Canada (Inuit Nunangat) including: Inuvialuit (NWT); Nunatsiavut (Newfoundland and Labrador); Nunavik (Quebec); and Nunavut. About 80 percent of Inuit reside across 53 communities within Nunangat (Inuit Tapiriit Kanatami, 2011). Inuit Nunangat encompasses about 35 percent of Canada’s landmass and 50 percent of its coastline (Inuit Tapiriit Kanatami, 2011). According to Inuit Tapiriit Kanatami, it is reported that about 60 percent of Inuit report speaking Inuktut (the Inuit language), and 76 percent of Inuit in Nunavut have Inuktitut as their mother tongue (Government of Canada, 2017). The focus of our chapter will primarily be Nunavummiut (Inuit residing in Nunavut) residing in the Qikiqtaaluq region of Nunavut. The Qikiqtaaluq region consists of 13 fly-in communities.
Pre-Colonialism with Qallunaat (Non-Inuit, Particularly of European Descent)
Consistent with all Indigenous groups at the time, Inuit had a thriving, holistic society and actively met their needs through economic, social organization, and spiritual connections. The economic connections centred on the power of Inuit to meet basic needs of food, shelter and clothing (Arctic Children and Youth Foundation [ACYF], 2018). Within traditional Inuit society and harsh climates, Inuit sustained themselves in their diet by hunting, harvesting and eating all of the animal—this provided a significant source of nutrients and needed sustenance. According to Inuit Tapiriit Kanatami (2011), social organization related to how Inuit organized their relationships with each other (e.g. gender roles, communication protocols, education, leadership, governance, dealing with wrongdoers, etc.) and it was intentional and practiced. The social organization allowed Inuit to have control and agency in day-to-day life. Spiritual practices revolved around the way that Inuit explained their existence through ideas of higher powers, rules of life, relationship with the natural world, and individuals acting as intermediaries with the spiritual world. There are several key historical events that greatly impacted upon the lives of Inuit, primarily colonialism.
1800s-Early 1900s
Whalers began to come to the area from England, Scotland and the United States, as products such as whale bones for corsets, and whale oil were in high demand (ACYF, 2018). Unlike explorers who were just passing through, whalers visited yearly and therefore had a bigger impact on the life of Inuit. According to the Qikiqtani Inuit Association (2013), whalers drew on Inuit knowledge; they employed, traded with, and socialized with Inuit. The relationship between whalers and Inuit introduced regular trade for things like flour, tobacco, textiles, and other metal tools; music such as square dancing (which Inuit still practice today); and social relationships, including babies born from unions between whalers and Inuit (Qikiqtani Inuit Association, 2013).
The first Hudson Bay Company (HBC) trading post was established in Kimmirut in 1912. This expanded to 100 trading posts in the North West Territories (NWT), although not all were HBC. Due to the influence of the trading posts, Inuit started hunting for trade, not just for food, and people grew more dependent on trade goods such as flour and tobacco. This shift caused families to become more individualistic throughout the North, and is seen as the beginning of the use of “money” for Inuit populations (ACYF, 2018). Inuit became dependent, then, on both money and goods, and when these were in low supply, they turned to government services for support.
Canadian Government and RCMP Impact on Inuit
The Royal Canadian Mounted Police (RCMP) initially came to the north in response to threats to Canadian Arctic sovereignty (American and European traders) in the early 1900s. RCMP began travelling to northern communities to enforce Canadian law. In traditional Inuit society, a system was already in place to deal with individuals who were out of line within the group: those who were troublemakers or who caused threats to others (Karetak, 2013). At that time, decisions would be made by Elders, hunters or the whole camp, for the betterment of the camp, and for the good of the group as a whole. This traditional justice worked for the unique lifestyles of Inuit. Increased confusion was created for Inuit with the involvement of RCMP and the new and unfamiliar ways of the Canadian justice system.
Relocation
At the time of the Cold War, many countries fought for sovereignty to claim the North, and Canada sent the military to the North to claim the land. The federal government moved, through forced relocation, the “Canadian Indians” (Inuit) further north in order to claim that land (Inuit Tapiriit Kanatami, 2004; Inuit Tapiriit Kanatami, 2011). At first, Inuit that moved from the Qikiqtaaluk region to higher latitudes (Grise Fiord) understood that they could return to their home communities if they chose. However, this return did not happen. Other relocations occurred with Inuit from northern Quebec, and many suffered greatly and/or died. Extreme weather, and distinct hunting patterns in the unfamiliar territory was the cause. The relocations created artificial settlements, which then turned into communities. On August 18, 2010 in Inukjuak, Nunavik, John Duncan, who was the Minister of Indian Affairs and Northern Development at the time, apologized on behalf of the Government of Canada for the relocation of Inuit to the High Arctic (Government of Canada, 2010).
Figure 1
Apology Statute in Grise Fiord
Tuberculosis in the North 1940s – 1960s
Around 1946, thousands of Inuit across the Canadian North suffered a severe outbreak of tuberculosis (TB). This occurred because of the increase in contact with people from southern Canada and the American military who were stationed in the North. The Canadian government sent a coast guard ship called the C.D. Howe to screen Inuit in the North. Members of the settlements were forced to board the ship and be screened for this and other diseases. However, any individual found to have any signs of TB was not allowed to get off the ship. In this way, children, women, and men of all ages were taken away from their families, and many never returned. The majority of Inuit did not speak English, and the southerners did not speak Inuktut, which affected communication. Inuit would spend an average of two and half years in the hospital due to the tuberculosis outbreak, and during this time, many who had left as children had forgotten their language and crucial survival skills. Most importantly, many individuals had missed out on valuable time with family. Some families to this day do not know the whereabouts of their members who died in TB sanitoriums (Olofsson et al., 2008). As a result, many Inuit lost their traditional connection to land and culture. At one point, one in every seven Inuit were in treatment in the south. By 1970, the long-term hospital treatments slowed the epidemic, but Inuit continue to suffer from TB. On March 8 2019, Prime Minister Justin Trudeau apologized to Inuit for the deliberate mistreatment of Inuit with TB; he committed funding towards travel costs for families who knew where their relatives were buried in addition to funding for marking graves and creating plaques (Government of Canada, 2019).
Residential & Federal Day Schools
Prior to colonialism, Inuit had their own way of educating their children. Because Inuit did not have a writing system, children learned through hands-on experiential learning and oral traditions, including the sharing of legends and stories teaching lessons. Residential schools began in the late 1940s for Inuit, and the children were sent away from their families to attend the schools in places far from their home. If Inuit refused to let their children attend, they would not receive or be eligible for the Federal Family Allowance program—this was the first universal welfare program for families. While attending the school, many children were physically, sexually and mentally abused, could not speak their mother tongue nor were allowed to engage in Inuit practices. The separation of children from their parents during these events severely-affected family attachments, ways of knowing, language, knowledge, communication and the foundation of Inuit kinship society (Healey, 2016). Throughout these atrocities, it was maintained that the schools were present to benefit Aboriginal communities (Macionis & Gerber, 2005). By 1964, 75 percent of Inuit children and youth aged six to 15 were enrolled in the schools (Pauktuutit Inuit Women's Association of Canada, 2007). The children who attended the residential schools lost their identity in many ways. The last residential school in Canada closed in 1996; however, the intergenerational trauma from attending residential school continues today. In 2008, then-Prime Minister Stephen Harper apologized to the victims of residential schools on behalf of the Canadian Government (Government of Canada, 2008).
Dog Slaughter
Dogs played an important role for survival for Inuit (i.e. hunting, travel and protection). In the 1950s and 1960s, it is estimated that 20,000 sled dogs were killed (Qikiqtani Inuit Association, 2013). The slaughter happened all across the Arctic yet was not known as a common occurrence because communities were spread apart, and communication was limited. An Inuit family coming into a town might have had their dog team slaughtered in order to force them to stay in the community. Elders have mentioned that this slaughter could also have been orchestrated to assist the Hudson Bay company (HBC) to sell their skidoos (Qikiqtani Inuit Association, 2013). Eventually, the skidoos replaced sled dogs, and Inuit started living in the communities rather than in small outpost camps. Traditionally, family groups would move to where the hunting was plentiful, but being forced to stay in one area meant that hunting was often less plentiful. Distrust towards the RCMP also began to emerge during this period. On August 14, 2019, then Minister of Crown-Indigenous Relations and Northern Affairs, Carolyn Bennett, apologized on behalf of the government of Canada for colonial practices imposed on Inuit, including sled dog killings—as well as the forced relocations and family separations—to the Qikiqtani Inuit (an Inuit organization representing the Qikiqtaaluk region) (Government of Canada, 2021).
Figure 2
Training Dog Team in Iqaluit, Nunavut
1970s to the Formation of Nunavut
Over the past century, Inuit have been attempting to regain their culture and identity through the work and advocacy of a multitude of local and national level organizations. The organization towards self-government is one example, and organizations that led that process included: 1971 Indian Brother of the NWT; 1971 Inuit Tapirisat of Canada (currently Inuit Tapariit Kanatami); 1972 Inuit Cultural Institute established; and 1981 Inuit Broadcasting Corporation. At present, Inuit Tapariit Kanatami is recognized as the national voice for Inuit of Canada. The role of Inuit Tapiriit Kanatami since its inception has been to support and advance Inuit right to self-determination and self-governance. Through coordination of Inuit Tapiriit Kanatami and its national committees, Inuit were able to secure inclusion of section 35 into the Canadian Constitution Act of 1982, which affirms First Nation, Metis and Inuit rights (Inuit Tapiriit Kanatami, 2004). Inuit Tapariit Kanatami represents four Inuit land claims organizations in Inuit Nunangat and include: Inuvialuit Regional Corporation, Makivik Corporation, Nunavut Tunngavik Incorporated, and the Nunatsiavut Government.
The Nunavut Land Claims Agreement (NLCA) is a landmark agreement with the federal government, which divided the NWT and created a new territory called “Nunavut.” Nunavut has 28 communities that cover 20 percent of Canada’s landmass and three time zones. Nunavut is separated into three regions (Kitikmeot, Kivaliq and Qikiqtaaluk). It came into being on April 1, 1999. The Legislature began with 19 Members of the Legislative Assembly (MLAs). The government is a consensus government, working for agreement among all its members that respected Inuit Qaujimajatuqangit (IQ) values (Government of Nunavut, 2007).
The incorporation of Inuit Qaujimajatuqangit (IQ) values into every aspect of modern-day practices within Nunavut exists to maintain and enrich the cultural heritage of Inuit. IQ values are therefore central to Inuit way of living and self-determination. The following IQ values are not only integral to the way of being in Nunavut but also encompass service provisions, such as providing service as a social worker.
Inuit Qaujimajatuqangit (IQ values)
- Inuuqatigiitsiarniq: Respecting others, relationships, and caring for people:
- Tunnaganariq: Fostering good spirits by being open, welcoming, and inclusive:
- Pijitsirniq: Serving and providing for family and/or community
- Aajiiqatigiinniq: Decision making through discussion and consensus
- Pilimmaksarniq/Pijariuqsarniq: Development of skills through observation, mentoring, practice, and effort
- Piliriqatigiinniq/Ikajuqtigiinniq: Working together for a common cause.
- Qanuqtuurniq: Being innovative and resourceful (i.e. in solving problems)
- Avatittinnik Kamatsiarniq: Respect and care for the land, animals and the environment
(Government of Nunavut, 2007)
The incorporation of IQ values into service mandates and programming is helping shift the way systems respond in supporting individuals and families within Nunavut. The complex history of Inuit reviewed in the previous section of this chapter has led to intergenerational trauma. Intergenerational or historical trauma refers to trauma experienced by past generations that continues to have an impact on descendants (Crawford, 2013). In many Indigenous communities, such as Nunavut, the presence and impact of intergenerational trauma is commonplace. In recognizing this intergenerational trauma, several initiatives and groups have been working towards a model of service delivery to the most vulnerable segments of the population. The incorporation of IQ values is central to providing appropriate provision of care, as it recognizes the importance of Inuit principles in addressing historical harm. As we transition to our case study, it is important to be mindful of the themes and concepts learned in the previous sections. The application of the previous learning will aid in our perspective with respect to providing care and support to the fictional young Jessica and her family.
Community Response to Care
In this section of the chapter, we will describe the local approach and support given to children and families like those identified in the case study. In the previous section we learned of the history of Inuit through colonialism and the role of national organizations in elevating Inuit voices. Furthermore, the introduction and incorporation of IQ values into programs and services is gradually changing the relationships that community members have to these services. For example, the initial contact for Jessica, following her disclosure, is important as her connection would not have been possible without services explicitly embracing IQ values. Rooted in IQ values is the Surusinut Ikajuqtigiit protocol. The application of this protocol in Nunavut has been able to shift how service providers support the most vulnerable children and adolescents in the community.
Surusinut Ikajuqtigiit (A Group Helping Children)
Based on generations of mistrust from governmental services and entities, forming meaningful relationships is crucial in remote communities such as Nunavut. Traditionally, the basis of strong relationships in Inuit culture has typically related to connection to family, friends and community with a level of equity. The sustained resilience of many Inuit can be attributed to horizontal ties, by which individuals have equal membership and there is reciprocity and cooperation. Vertical ties are relationships in which a member has greater standing with respect to authority, knowledge and wisdom (Brown, 2020). Increasingly, as southerners and governments use vertical ties in their relationship to Nunavut, the sense of belonging and acceptance for Nunavummiut becomes revoked. Vertical ties can be instrumental in some aspects of social work practice; however, when the power balance misaligns, it can become detrimental to the culture, values, and rhythm of the community. Therefore, any collaboration must adhere to traditional community principles as a priority, and must be both reflective and reflexive of generational harm inflicted on individuals and communities by southerners. As social workers, we need to be mindful of the distinction between horizontal and vertical ties. An equitable relationship at the horizontal level can eventually inform the expertise that may be sought at the vertical level.
The creation of Surusinut Ikajuqtigiit (SI) policy as led by governmental departments in Nunavut, is based on the eight IQ values identified earlier in this chapter. Surusinut Ikajuqtigiit recognizes the importance of collaboration (Piliriqatigiinniq—working together for a common cause) within the care provided to the most vulnerable populations. The policy was achieved through active collaboration with governmental organizations who are normally responsible for the care, safety, and education of children and adolescents. The collaboration between these governmental departments, non-governmental organizations, and Elders responding to the needs of the child/adolescent and family is the foundation of SI by protecting children and ensuring that their voices are heard. SI emphasizes the need for multi-disciplinary approaches, collaborative and responsive practices, promotion of child-centred and strength-based investigations, and support services to children and youth. Without the collaboration of community members and important policies as laid out in SI, the creation of coordinated services such as Child Advocacy Centres would not exist (Government of Nunavut, 2020).
The incorporation of SI and IQ values are examples of appropriate connection between horizontal and vertical ties. Simply, if there had not been significant engagement at the horizontal level through engagement and relationship building, it would be very difficult for the community to have embraced other systems. Similarly, the creation and success of Child Advocacy Centres (CACs) is attributed to an appreciation of ties. Without one service provider willing to acknowledge their limitations to another organization with mutual interests, services would be fragmented, and would not take into account the best interest of an individual or community.
Child and Youth Advocacy Centres
Child Advocacy Centres (CACs) or Child and Youth Advocacy Centres (CYACs) exist in support of children and youth who have experienced different forms of abuse/maltreatment (Hickey, 2015). CACs/CYACs provide child-centred environments for the person receiving support. Although the CAC model may have variations across regions, it is recognized as an overall best practice model of care for response to child/adolescent abuse (Bertrand et al., 2018). The Centres are created out of a need to improve disjointed service collaboration and lack of child-centred processes, which inevitably causes more trauma to a child after abuse/maltreatment. As highlighted in Table 1, CAC/CYACs have been shown to have many short- and long-term benefits (Bertrand et. al., 2018; Herbert & Bromfield, 2016).
Table 1
Benefits of CACs
| Short Term Benefits | Long Term Benefits |
|
|
Note. Adapted from Herbert and Bromfield, 2016.
CACs in Nunavut
It is reported that child abuse and maltreatment rates in Nunavut are approximately 10 times that of the national average (Representative of Children and Youth, 2019). The stark difference in these rates has resulted in a demonstrated need for improved service coordination in Nunavut to support children and adolescents. Based on a community needs assessment, it was determined that a CAC would provide supports using a child-centered, culturally-relevant response to young Nunavummiut (people residing within Nunavut) who have experienced child abuse and neglect (Qaujigiartiit Health Research Centre, 2010). The embracing of a CAC in Nunavut was encouraged through service partners in the creation of the SI.
With the non-governmental organization (NGO) Arctic Children and Youth Foundation (ACYF) as lead, the following organizations and departments were involved in the collaboration: Justice, Health, Education, Child and Family Services, the RCMP, and Nunavut Tunngavik Incorporated (NTI). These organizations signed a memorandum of understanding (MOU). An MOU is an agreement between distinct parties with mutually-accepted expectations. The expectation was the commitment of the highlighted parties to create a CAC in Nunavut where children and their families can feel safe and comfortable to access support.
The Umingmak Centre became operational in 2019 in Iqaluit, Nunavut. Since opening, the Umingmak Centre has provided services and resources to children and families where there have been disclosures or suspicions of crime relating to abuse (i.e. exposure to significant caregiver violence, death and homicide, sexual abuse, neglect and physical abuse). The Centre uses best practice in child abuse investigations, assessment, support and treatment by coordinating with its service partners (e.g. RCMP, Child and Family Services, Pediatricians, Justice, Education and allied community members).
Umingmak is the Inuktitut word for muskox. Umingmaks are known to be very protective of their young. When a young umingmak is in danger, the adults create a protective barrier around them to shield them from harm. The analogy of protection is rooted in the purpose of the centre and community values around caring for vulnerable children and adolescents.
Figure 3
Umingmak Centre
The Umingmak Centre has highly skilled professionals who provide quality service through a trauma informed lens with children/adolescents and their families.
Roles at the Centre
To help describe how a CAC works, and how it might serve the needs of someone like Jessica in our case study, we will describe the role of each member of the team at the CAC.
Child/Adolescent Advocates at the Umingmak Centre are responsible for supporting children/adolescents, and their non-offending caregivers with age specific trauma informed support. Advocates are the main point of contact for children and non-offending caregivers. They are ultimate service and system navigators following the completion of the interview or investigative process and are a source of psychoeducation to families and children/adolescents.
The role of the Inuit-trained Counsellors at the Centre is to support families, children/adolescents through trauma-informed information and supports. The Inuit counsellors utilize a combination of both western and culturally based approaches. The counsellors also practice from the perspective of IQ principles. Counselling can occur in the context of individual, family and group formats. Given the disruptive nature of trauma in a family setting, family therapy allows individuals to incorporate the various available resources. With cultural and individual family considerations, family therapy can include whoever the child/adolescent views as a supportive person. Counselling can be tailored to individual needs.
The Umingmak Centre works closely with local Pediatricians. The role of the pediatrician is to provide clinical support in the investigative process, and to complete a forensic examination (collect DNA samples from child/adolescent for testing and provide essential medical care). Pediatricians also provide reassurance examination for cases where there has been a historical disclosure (disclosure that occurred outside clinical limits for examination). They also meet with the child/adolescent and their non-offending caregiver as needed in order to provide follow-up care. The Centre works closely with specially trained RCMP Interviewers in child/adolescent cases of maltreatment called the Specialized Investigation Team (SIT). The SIT was formed in 2019 as part of the Nunavut RCMP V Division. The SIT is focused on assisting and conducting investigation of sexual crimes involving children and adolescents across the territory of Nunavut. The officers will typically conduct their interview in plain civilian clothing to reduce stress and intimidation possibly triggered by the uniform. For many children/adolescents who have been interviewed at the Centre, it is typically the first time seeing an officer in civilian clothing. The interviewer’s role is to acquire as much information relating to the disclosure as possible in order to determine if a charge can be made.
The role of the Child Protection Worker is essential to the investigative process of the particular allegation/charge, and ongoing after that time as needed, to ensure the safety of the child/adolescent. Protection Workers are also known as Social Workers within Nunavut. Protection Worker will typically bring the family to the Centre observe the interview for further interventions and provide support as well. Simultaneously observing the interview eliminates the need for further interviews which might be distressing or retraumatizing.
Case Study and Multidisciplinary Care
Now that we have reviewed the history of Inuit in Nunavut and the CAC model, we can look at how this multidisciplinary care would look for Jessica from our case study. We will review the steps and process of investigation typically followed in Nunavut, as well as the start of healing for Jessica and her family. We learned earlier that the creation of the Surusinut Ikajuqtigiit (SI) policy was to encourage collaboration following disclosures of abuse. Disclosures of childhood sexual abuse within Nunavut typically are received through Child Protection Services and the RCMP. As part of the SI, there is an emphasis on the importance of community partners ensuring that their efforts to protect children from abuse are integrated, effective, and culturally appropriate.
Each of the smaller communities in Nunavut has a Community Health Centre (CHC). Community Health Centres provide a variety of health services (i.e. emergency, pre-and post-natal, immunizations, public health, counselling, mental health and etc.) and are typically supported by community members and nurses. In the Qikiqtaaluk region, physicians typically fly into the community on a rotational basis every few weeks. Nursing staff connect with physicians via phone or email (depending on urgency) to best support clients locally. For more complicated or urgent cases, the individual is flown to Iqaluit via scheduled flights or medevac (air ambulance).
In this fictitious case of Jessica, her disclosure activated different reporting agencies within her community of Kinngait. Upon being examined by the Community Health Nurse (CHN) at the Health Centre, the CHN had to contact Child Protection Services as part of her Duty to Report, as well as the RCMP. As we have previously learned, Child Protection is responsible for the safety of the child/adolescent and will determine if the child needs protection, whereas the RCMP investigates to determine if criminal charges are to be laid.
Due to the time sensitivity in the case of Jessica, the CHN sought direction from the physician who was on call in Iqaluit. Based on the physician consultation, the decision was made to have Jessica flown to Iqaluit for further care. A full investigation was not possible in the community due to the timing of the scheduled plane arrival, so both Child Protection Services and the RCMP made sure to connect with counterparts in Iqaluit.
Jessica Arrives in Iqaluit
In the case study focusing on Jessica, arrangements were made with Child Protection Services to provide the family with transportation at the airport. As the flight arrived late, the Child Protection Worker ensured that the family was taken to the local medical hotel/boarding home for individuals and families visiting Iqaluit for medical care. Arrangements were subsequently made with Jessica and her mother to be picked up in the morning to come to the Umingmak Centre.
Upon arriving at the Umingmak Centre, Jessica and her mother Tapisa were welcomed by the Advocate who is Inuk (singular for Inuit). At the onset of the therapeutic relationship, the Advocate typically provides a tour of the Centre to the child/adolescent and their non-offending caregiver, as was the case for Jessica and Tapisa. The Advocate reinforces the existing supports and highlights that the Centre is dedicated in building community relationships and resources to help families throughout the journey from disclosure to healing.
Often country food (food that is local to Inuit) and beverages are offered and shared during this time, which is consistent with Inuit culture. The experience can at times be quite overwhelming for non-offending caregivers as many caregivers are flooded with emotions about their own past traumatic experiences. As we learned earlier in this chapter, the impact of intergenerational trauma is pervasive within northern communities. Being in supportive spaces like the Centre can at times result in many caregivers disclosing their own experience of abuse (typically sexual maltreatment) during the introduction meeting with their child/adolescent. Caregivers of children/youth involved with the Umingmak centre have been universally thankful for the existence of services through the Centre for their child/adolescent, but often talk about the contrast in the potential impact that the Centre’s existence would have had within their own adult lives and healing had it existed for them during their childhood. As needed, the Centre typically connect caregivers to an Inuit Trained Trauma Counsellor.
Specialized Investigative Team (SIT)
Jessica was introduced to two female members of the RCMP SIT who conducted her interview. Typically, one will lead the interview and the other will monitor the interview in another room along with the Child Protection Worker. Jessica is bilingual (fluent in Inuktitut and English), but preferred to be interviewed in English, and therefore was interviewed by an English-speaking interviewer. In the event that Jessica was unilingual in Inuktitut, an Inuktitut speaking RCMP member would have taken the lead on the interview, or an interpreter would have been provided. In Nunavut, there has been significant recognition for the need to train additional RCMP officers who are fluent in Inuktitut.
Medical Examination
Jessica was then introduced to the pediatrician. The pediatrician spent time with Jessica and her mother prior to the exam, to allow them to feel comfortable and ask questions. The clinic room is child friendly and is similar to any other clinical exam room in a community health centre or hospital setting. The pediatrician provided a medical assessment, which in this case included a forensic examination and obtaining forensic evidence with a sexual assault evidence kit (SAEK). The specifics around evidence collection were provided by the forensic interview that was completed. With consent, Jessica’s mother was present for the entire examination.
Case Review
Following the interview with Jessica, the SIT members met with the pediatrician to review their respective interviews and assessments. In this case, there were significant findings by the pediatrician during the examination. It was also helpful that Tapisa kept Jessica’s clothing from the sexual assault which was then sent out for testing. The majority of sexual assault evidence collection is sent to Manitoba to the RCMP national forensic lab for testing. During this review, the SIT lead investigator also confirmed that Jessica gave a disclosure, which resulted in her uncle being arrested and charged.
Following this discussion, the SIT members, pediatrician and advocate met with Tapisa and Jessica to inform them about next steps. Tapisa became emotional after learning about the disclosure and medical findings. Tapisa expressed worries about being evicted from the familial home as it is owned by her brother (the alleged perpetrator). The team attempted reassurance that the support Jessica has received will be a big factor in determining the positive healing journey ahead for her. Victims of sexual abuse have better treatment outcomes if they feel believed by the person they disclose to (Humphreys, 1992; Vaplon, 2015). Tapisa was offered additional support through the Inuk Trained Counsellor and also met with the Child Protection Worker to develop a safety plan.
At this point, an exploration of a treatment plan was reviewed with the multidisciplinary team at the Centre. Typically, for cases within the Qikiqtaaluk region, interdepartmental collaboration occurs and families are supported to travel and have ongoing support in their home community (i.e. Mental Health Nurse, Outreach Worker, Wellness Counsellor and in some cases an Elder).
In the case of Jessica, following the immediate arrest of the uncle, Tapisa, Jessica and their family were evicted from the home. This created an emergency situation of homelessness. According to Inuit Tapiriit Kanatami (2014), about 39 per cent of Inuit in Inuit Nunangat live in overcrowded homes compared to four percent of all Canadians. The significant disparity can create additional stressors and pressures for families fleeing violence. In the case of Jessica, the Protection Worker was able to make arrangements to have Tapisa and her children brought to Iqaluit for emergency housing. Nunavut operates family violence shelters in each of the three regions.
Healing Considerations
The deleterious long-term impact of child maltreatment and trauma for children/adolescents often manifests in the breakdown of family systems and poor psychosocial outcomes (Buss et al., 2015). Within treatment, the goal is recovery for the individual, family and caregivers. At the Umingmak Centre, individual trauma counselling is available for children and youth who meet criteria for counselling along with their non-offending caregivers. The treatment program provides principles of trauma-informed practice which highlight the principles of trust, safety, choice, and control. The goals of the programs are to reduce the negative impacts of abuse, trauma, and maltreatment while fostering resilience. Each client’s treatment plan is created collaboratively with the client and the multidisciplinary team, as the ultimate goal is to allow the child to heal holistically in the domain of the physical, developmental, cultural and spiritual self.
Being believed by a non-offending caregiver, following disclosure of abuse, can at times be transformational for the child/adolescent providing the disclosure (Bolen & Lamb, 2004; Humphreys, 1992). Simply, within the therapeutic process, non-offending caregivers possess the ability to play an essential role in supporting their child/adolescent through traumatic disclosures and subsequently the experience itself. In keeping with the importance of familial relationships among Inuit, there is active mobilization of the child’s support systems. The additional recognition of the non-offending caregivers highlighting their own historical and sometimes active traumas, can at times complicate the healing journey for the family, particularly the child/adolescent (Manion et al., 1996). The complexities of supporting the family system through a culturally-centric approach in helping members of the family heal in their recovery journey, specifically focusing on the challenges facing the non-offending caregivers and their respective traumas, is quite significant. The role of the Inuit Trained Trauma Counsellors assists in making this work successful
Multidisciplinary teams can be incredibly helpful for families such as Jessica’s in navigating their healing journey through the linking of services and resources available within the community. Although, discussion and actions coming from these teams’ meetings will look different for every child/family, the collaboration of partners remains essential in better understanding and meeting the needs of each child.
The well-being of children is impossible to separate from the well-being of their caregivers and others within their community (McKenzie et al., 1995). Within the literature it is well understood that non-offending caregiver support typically has four major dimensions: believing the child, protecting the child, emotionally supporting the child, and obtaining resources for the child (Priebe & Göran, 2008). The shame associated with sexual abuse is at times amplified in remote communities such as Nunavut. As the child/adolescent moves through their trauma healing, the objective is to create new narratives which will empower them to reconnect with previous joys and normalcy within their lives and community. Part of this reconnection centres around family and strengthening the bond associated with same. In collaboration with the family, the Centre is actively finding ways of incorporating traditional healing (i.e. on the land programming) to increase the reconnection for the child/adolescent. Additionally, part of the healing includes increasing the child/adolescent’s cultural identity through mentorship with the Inuit Advocates at the Centre. For Jessica this includes learning about her own Inuit history through the experience of running a dog team or being part of therapeutic groups with peers who have had similar experiences.
Figure 4
Being on the Land
Levels of Social Work Practice in Nunavut
Now that we have described a case scenario, we will dissect the levels of social work practices in Nunavut, while keeping this case in mind.
At the micro level it is important to recognize some of the barriers that individuals and families have to services. Clients like Jessica and her family received a variety of supports including individual, family and group therapy that was individualized to their specific needs. Within this work, clients are actively referred to other services within the community in order to achieve their full potential and healing needs. The involvement or exclusion of families within the therapeutic relationship at the micro level can also instill or breakdown further issues at this level. Being a social worker within a remote community such as Iqaluit is more than simply providing service and linking people to services. The role and responsibility has many important considerations, especially when working with vulnerable populations. Social workers need to be mindful of the generations of harm and the perpetual continuation of this within systems. More importantly the level of power and trust at the micro level needs to be respected and recognized when navigating larger systems with families.
As social workers, our work with clients at the meso practice level typically involves participation in working groups and advocacy towards achieving equitable services within the community. An example of this includes the formation of the Arctic Child and Youth Foundation (ACYF), which was founded by community leaders such as the current Governor General of Canada, Mary Simon. In 2003, along with other community members, Mary Simon created the organization ACYF to support children and youth of Nunavut to navigate their quickly changing world from the traditional Inuit way of life. About a decade later, the prevalence of childhood sexual abuse was becoming even more apparent, and leading community members created a working group to address this important issue. The first Child Advocacy Centre (CAC) in Nunavut is an example of the gradual grassroots movements to address community issues at the meso level. Families, like Jessica’s, are able to receive coordinated services as a result of organization at the meso level.
Similar to the working group in the meso system, it took a couple of community leaders to focus on changes at the macro practice level. As a result of their efforts over the past two decades, change have occurred at the political level by having a Memorandum of Understanding (MOU) created within all the departments in Nunavut who are responsible for the well-being of children, such as Education, Health, Justice, Child and Family Services, the RCMP, and Nunavut Tunngavik Incorporated (NTI). The support of leaders from these departments for this MOU has allowed the opportunity for there to be a focus on children and adolescents in Nunavut to receive the coordinated, consistent care they deserve with respect to adverse experiences such as abuse and maltreatment. The opening and subsequent success of the Umingmak Centre has also encouraged governmental and non-governmental funders to create a second CAC within the Kitikmeot region of Nunavut.
Without the advocacy of social workers, allied professionals and community members doing individual and family interventions and then shinning a light to the important and prevalent issue of child abuse, there would have been no working groups, political will and data collection to support the need of a transformative approach to addressing child abuse in Nunavut. The collaboration of these leaders would not have been possible without the ability to contextualize the issue of abuse and the manifestation of it as evidenced by significant harm inflicted on the community following colonization. Community members actively recognized the impact of the historical harm and transformed it through an adherence to Inuit Qaujimajatuqangit (IQ) values, working collaboratively across sectors for the betterment and future of the most vulnerable populations.
Ethical Considerations for Working in the North
Living and working within a northern, remote setting such as Nunavut makes it challenging for one to truly understand and appreciate the context. Specifically, there is a strong foundation of culture and experience in each community that requires respect from workers who come from outside those communities. Therefore, social workers should be proactive in increasing their overall knowledge, prior to working in such a setting. Furthermore, respect, humility, and openness to learning are essential and the genesis of these principles do not begin once you are in the setting but prior. Professional development allows for this crucial foundation for social workers entering practice in a northern community. Without the provisions outlined in social work codes of ethics, the manner in which professionals conduct themselves could adversely affect not only the worker but the type of work done with vulnerable clients and their families. An adherence to regulated bodies such as a college of social work can ensure that the work is being guided with the best interests of our clients, especially in marginalized and vulnerable communities in Nunavut. In stating this, our clients are left at a disadvantage when we engage in the work without any accountability through connection with a regulated body. Currently, in Nunavut, there is no mandate to be part of a college of social workers, which can lead to concerns especially when the individual is a new graduate. Ideally, a competent social worker is guided by legislation so that they are better able to work within those parameters or possibly challenge policies. When practitioners do not have a professional college to belong to, this can create issues with appropriate checks and balances, which can leave the client in a situation with limited recourse if ethical violations occur. In remote communities such as Nunavut, having a professional college affiliation is essential when considering the history of harm.
Although professional membership is not mandatory, many social work practitioners in Nunavut have opted to be part of the Association of Social Workers in Northern Canada (ASWNC). The ASWNC represents social workers in the Yukon, Northwest Territories and Nunavut. The aim of the Association is to provide support to social workers through professional development and representation at the territorial and national level. The values in the Code of Ethics adhered to by ASWNC follows that of the Canadian Association of Social Workers (2005), which includes: respect for the inherent dignity and worth of persons; pursuit of social justice; service to humanity; integrity in professional practice; confidentiality in professional practice; and competence in professional practice.
The issues that arise in northern social work practice include practicing beyond our competence, dual relationships, having too much access to information, and limited supervision. An additional issue is professional drift which can occur in northern communities where a social worker can abandon the purpose associated with the profession in place of roles associated with other disciplines. The role of a regulatory body would be to ameliorate the emergence of such issues by keeping social workers within the boundaries of their profession. Although there is no regulatory body within Nunavut, practitioners are still morally obliged to uphold these standards and adhere to these boundaries through membership involvement and appropriate supervision. When practicing in northern and remote communities, the lack of resources or “experts” within communities can result in many social workers engaging in work that is normally outside their expertise, or a practicing social worker might align oneself with the practice of other professionals within the community (Schmidt, 2009). For instance, a social worker might be asked to assist with a role outside their usual scope, simply due to a shortage of staff. Although well intentioned, this alignment may lead to service and care that is not client centred. Social workers who embrace these additional roles for the sake of resource scarcity also risk denying clients their right to feel empowered. Due to the nature of social work practice in the north, we are also privy to more details of our clients’ personal lives, as we are neighbours with our clients; we see them at the grocery store and at the hockey rink. This familiarity is not the case in other geographical settings. Truly, the combination of these factors places us in various ethical predicaments.
For social workers in northern practice, appropriate supervision is essential in ensuring that the described challenges are avoided. In balancing a client’s right to self-determination along with an ethical dilemma, the role of a culturally-diverse multidisciplinary team is even more important in all decision-making processes.
As social workers, our professional knowledge, insight and experience allow clients to work with us and hopefully trust us. If barriers exist to us upholding that professionalism, this may impact our ability and growth as a social worker, which in turn will negatively impact clients. Any regulatory body for our professional code of ethics is a reference point that allows us to do the work that we are intended to do within this helping profession. Furthermore, our removal from this process, or lack of acknowledgement of the historical context, would be harmful not only to our therapeutic relationships but also to the growth experienced by our clients.
Challenges and Barriers
Geography poses the most significant barrier to families and their ability to access professionals, including social workers. Finances for physical travel are obvious, but the latent barriers geography poses for families are perhaps more dangerous to meaningful access. The implications of Jessica and her caregiver travelling some distance for care outside her home community are significant. Without access to childcare, families with a child/adolescent in need of medical practitioner care, as well as care from allied professionals (including social workers) at a Child Advocacy Centre (CAC) may be forced to choose between accompanying the child to the CAC and leaving remaining children in non-ideal child care arrangements or in the temporary care of a child welfare agency. In addition to child care issues, accessing care may mean parents are forced to choose between taking unpaid leave from work and forgoing wages needed to feed and house their families. As social workers in remote communities, we need to be aware of these realities, as they provide essential context to any client intervention and goal setting. Awareness of these realities also ensures that we manage our expectations of our clients by not asking too much of them.
The reality of the case of Jessica highlights many inequities that continue to exist for victims of child abuse and family violence. Limited availability of resources typically means that the victim has to relocate in order to access support. In some instances, the abuse is maintained and perpetrated as the victim(s) are unable to leave, and there are no emergency resources within the community. The daunting reality faced by families like Jessica’s present additional stressors and systemic barriers for families in their healing. In this situation, following the disclosure, Jessica had to travel out of her home community for additional care and supports. Jessica also learned that, as a result of her disclosure, she and her mother were no longer welcome in their familial home. As the family considered these new changes, Jessica and her siblings also had to consider changes to their home environment, social life and emotional supports. Tapisa also has to be able to navigate new employment and support systems for herself and her family.
The challenges facing the child/adolescent in a remote community in Canada are evident and need to be acknowledged. Southern social workers in remote communities such as Nunavut need to understand the barriers in place and how these barriers may affect children and families. This understanding will help social workers and allied professionals in connecting and supporting families successfully at micro/meso/macro levels. As seen by the progression of grassroots organizations, no social worker or medical practitioner is going to change the world overnight. Rather, the role is to understand and chip away at the challenges that have been cemented through generations of trauma and wrong-doing. Understanding the community, knowing the families and their challenges, understanding the available resources and the lack of resources facing families, and listening to concerns is crucial to transformational and meaningful change.
In addition to understanding children/adolescents, their families, and the communities from which they come, it is extremely important that social workers from the south operate from the perspective of diligently making connections and knowing what resources are locally available. Whether it is the Community Health Nurse (CHN), the Child Protection Worker, a community justice worker, a government representative, or an Elder, such individuals will understand family dynamics, relationships, and any existing trauma far more than someone operating from a stand-alone place of “expertise.”
Conclusion
Inuit have lived in the Arctic region for over 5000 years and are the original inhabitants (Inuit Tapiriit Kanatami, 2004). Prior to colonization, Inuit resided in small, family-based camps, and were nomadic, travelling seasonally on the land for hunting, fishing and gathering all their food and resources. To survive the harsh climate, Inuit typically depended on each other to meet their basic physical needs (i.e. food and shelter). Established values sustained families throughout these hardships, and the resilience of Inuit has sustained them over the years. The role of Inuit Qaujimajatuqangit (IQ) values have also been instrumental in the maintenance of culture and identity. Furthermore, the incorporation of IQ values in policies and organizations has proved beneficial in the lives of Inuit, but this is an active process and practice, especially for southerners working in Nunavut with children/adolescents and their respective families.
As experts working in remote communities such as Nunavut, it is our duty to be informed about the histories and oppressions experienced by our clients. The deleterious long-term impact of child maltreatment and trauma for children/adolescents often manifests in the breakdown of family systems and poor psychosocial outcomes (Buss et al., 2015). The discovery of a child experiencing severe maltreatment can cause trauma to each family member, and can have serious implications for the lives of all family members. How a parent responds to a child disclosing abuse can also have a dramatic influence on the child. In a territory such as Nunavut, with a well-documented history of intergenerational trauma, social and physical inequalities, the impact of a disclosure in the family is typically experienced differently in that the dynamic shift can be significant (Representative for Children and Youth, 2019). Multidisciplinary teams can play a significant role in the healing of families, especially when the team is representative of the uniqueness of the community and its needs.
Based on the two decades of commitment towards the realization of the first CAC in Nunavut, it is easy to appreciate the complexity and challenges of historical harm. The Umingmak Centre plays the vital role of supporting children/adolescents with disclosures of abuse (e.g., sexual, physical, neglect and exposure to violence). The multidisciplinary approach is rooted in recognition of cultural perspectives and understanding of the initial disclosure and healing journey. Based on the uniqueness of the remote community, services available to the children and their respective families are fostered and enriched from a cultural perspective by creating allies within the community along with fostering service partnerships.
In supporting a child/adolescent in their healing, family involvement must be central to the child/adolescent’s overall recovery. Childhood sexual abuse is relational by nature, and therefore the importance of aligning with families to foster further healing through social learning and corrective narratives has the potential to sustain wellness within families. Increased connection and support is key to increased family empowerment, healing, safety, sense of self and resilience, and reduced generational transmission of trauma response.
Daniel A. Afram: As an African-Canadian social worker, I am aware of my own experiences of oppression and acknowledge this within other spaces of equity deserving people with shared struggles. This encourages me to engage in active reflexivity when working with and within Indigenous communities. My commitment to respecting the values and needs of Inuit, is founded on intentionality, active listening, and ongoing learning.
Amber Miners: I have reflected extensively on my own background and lived experiences. I am cognizant of the advantages and disadvantages these things have had, and continue to have in my life. I am perpetually working towards being more aware of my positionality within my community, the world and most importantly in relation the people I interact with daily.
Activities and Assignments
- If you were to start planning to open a CAC in a northern community close to where you are now, whom would you speak to first, and what would be your priorities in planning? Apply the concepts of micro, meso, macro perspectives to your answer.
- You are starting a new job in Kugluktuk, Nunavut as a social worker. You have recently graduated and are very keen. What do you expect will be your three biggest challenges, and how might you overcome those challenges?
- As part of your self-care, you have joined an extracurricular activity playing frisbee. One of your teammates is a parent of a family that you are involved with at work. How would you navigate this interaction?
- A caregiver you are supporting informs you that she is worried about a case conference at their child’s school. How would you apply the Surusinut Ikajuqtigiit in this situation to ease her worries about the meeting?
- This chapter highlighted the many challenges experienced by Jessica in leaving her home community to receive service. As the social worker helping the family with their transition to their new community, which IQ values will you apply to guide this process?
References
Arctic Children and Youth Foundation. (2018). Caring for others, caring for ourselves: Trauma awareness for young leaders.
Bertrand, L.D., Paetsch, J.J., Boyd, J.P., & Bala, N. (2018). Evidence supporting national guidelines for Canada’s child advocacy centres. Government of Canada, Department of Justice.
Bolen, R. M., & Lamb, J. L. (2004). Ambivalence of nonoffending guardians after child sexual abuse disclosure. Journal of Interpersonal Violence, 19(2), 185-211.
Brown, G. (2020, July 14). Difference between horizontal and vertical relationships. Difference Between Similar Terms and Objects. http://www.differencebetween.net/business/difference-between-horizontal-and-vertical-analysis/
Buss, K. E., Warren, J. M., & Horton, E. (2015). Trauma and treatment in early childhood: A review of the historical and emerging literature for counselors. The Professional Counselor, 5(2), 225-237.
Canadian Association of Social Workers (2005). Code of ethics. https://www.caswacts.ca/files/attachements/casw_code_of_ethics.pdf
Crawford, A. (2013). The trauma experienced by generations past having an effect in their descendants: Narrative and historical trauma among Inuit in Nunavut, Canada. Transcultural Psychiatry, 51(3).
Government of Canada. (2008, June 11). Statement of apology to former students of Indian Residential schools [press release].
Government of Canada. (2010, September 15). Apology for the Inuit High Arctic relocation [press release].
Government of Canada (2017, October 25). Census in Brief: The Aboriginal languages of First Nations people, Métis and Inuit.
Government of Canada. (2019, March 8). Statement of apology on behalf of the Government of Canada to Inuit for the management of the tuberculosis epidemic from the 1940s-1960s [press release].
Government of Canada. (2021, August 12). Minister of Crown-Indigenous Relations delivers apology to Qikiqtani Inuit [press release].
Government of Nunavut. (2007). Inuit Qaujimajatuqangit Education Framework for Nunavut Curriculum. https://www.gov.nu.ca/information/inuit-societal-values
Government of Nunavut. (2020). Surusinut Ikajuqtigiit: Nunavut Child Abuse and Neglect Response Agreement.
Healey, G. (2016). (Re)settlement, displacement, and family separation: Contributors to health inequality in Nunavut. The Northern Review, 42, 75-96.
Herbert, J. L., & Bromfield, L. (2016). Evidence for the efficacy of the child advocacy center model: A systematic review. Trauma, Violence & Abuse, 17 (3), 341–357.
Hickey, S. (2015, July). Child advocacy centres and child and youth advocacy centres in Canada: National operational survey results. Research and Statistics Division, Department of Justice Canada.
Humphreys, C. (1992). Disclosure of child sexual assault: Implications for mothers. Australian Social Work, 45(3), 27-35.
Inuit Tapiriit Kanatami. (2004). 5000 years of Inuit history and heritage. https://www.itk.ca/5000-years-inuit-history-heritage/
Inuit Tapiriit Kanatami. (2011). Inuit regions of Canada.
Inuit Tapiriit Kanatami. (2014). Comprehensive report on the social determinants of Inuit health. https://www.itk.ca/social-determinants-comprehensive-report/
Karetak, J. (2013). Conversations of Inuit elders in relation to the Maligait (Inuit laws). Nunavut, Department of Education.
Macionis, J. J., & Gerber, L. M. (2005). Sociology (5th ed.). Pearson Education Canada Inc.
Manion, I. G., McIntyre, J., Firestone, P., Ligezinska, M., Ensom, R., & Wells, G. (1996). Secondary traumatization in parents following the disclosure of extrafamilial child sexual abuse: Initial effects. Child Abuse and Neglect, 20, 1095–1109.
McKenzie, Seidl, E., & Bone, N. (1995). Child and family service standards in First Nations: An action research project. Child Welfare, LXXIV(3), 633–654.
Olofsson, E., Holton, T., & Partridge, I. (2008). Negotiating identities: Inuit tuberculosis evacuees in the 1940s-1950s. Inuit Studies, 32(2), 127–149.
Pauktuutit Inuit Women’s Association of Canada. (2007). Sivumuapallianiq: National Inuit residential schools healing strategy: The journey forward. Pauktuutit Canada.
Priebe, G., & Göran, C. (2008). Child abuse & neglect child sexual abuse is largely hidden from the adult society: An epidemiological study of adolescents’ disclosures. Child Abuse & Neglect, 32 (12), 1095-1108.
Qaujigiartiit Health Research Centre. (2010). Needs assessment of child and youth mental health services in Nunavut. Qaujigiartiit Health Research Centre.
Qikiqtani Inuit Association. (2013). Qikiqtani Truth Commission final report: Achieving Saimaqatigiingniq. https://www.qtcommission.ca/sites/default/files/public/thematic_reports/thematic_reports_english_final_report.pdf
Representative for Children and Youth. (2019). Our minds matter: A youth-informed review of mental health services for young Nunavummiut. https://rcynu.ca/sites/rcynu.ca/files/RCYO_MHReview_EN.pdf
Schmidt, G. (2009). What is northern social work? In R. Delaney & K. Brownlee (Eds.), Northern and rural social work practice: A Canadian perspective (pp. 1-17). Lakehead University Centre for Northern Studies.
Vaplon, C. S. (2015). The effects of parental response on their children’s trauma experience [Master’s thesis, St. Catherine University]. Sophia.
Photo taken in the summer months of August 2020 by Kylie Aglukark.
The focus of this chapter is on the changing landscape of rural and northern communities in Canada as a result of newcomer settlement in these locations; and on the role of social work in responding to the diverse challenges and opportunities facing these newcomer populations and their receiving communities. The definition of rural and northern being used includes both distance away from the cities or urban centres (spatial) as well as population size of communities (Johnston, 2020; Laurin et al., 2020). The terms settler and immigrant settler are used interchangeably to refer to newcomers who have moved to Canada from other countries. The term “settler” is intentionally used to push readers to keep Canada’s history of colonialism uppermost in mind during the discussions about newcomers in Canada. The chapter recognizes the presence of diasporic peoples who may have once arrived as immigrants but who are now settled as Canadian citizens, and for whom the term “immigrant” is no longer appropriate. This chapter also includes a focus on individuals arriving as refugees who are also seen as newcomers settling in Canada. The chapter recognizes the diverse ways in which newcomers or settlers are able to enter the country (Government of Canada, 2021). The list of pathways includes:
- Express entry (applications are reviewed based on three economic immigration programs: the Federal Skilled Worker, the Federal Skilled Trades Program, and the Canadian Experience Class).
- Family sponsorship
- Provincial Nominee Program
- Quebec-selected skilled workers
- Atlantic immigration pilot
- Caregivers Program
- Start-up Visa (opportunities to start a business or create jobs)
- Self Employment Program
- Rural and Northern Immigration Pilot: (several communities in Alberta, British Columbia, Manitoba, Ontario, and Saskatchewan are participating in this pilot).
- Agri-Food Pilot (opportunities to work in agri-food industries and jobs)
- Health-care workers permanent residence pathway
- Temporary resident to permanent resident pathway
- Permanent residence pathways for Hong Kong residents
In addition to the above, individuals applying as refugees may qualify for entry under the Economic Mobility Pathways Pilot (Government of Canada, n.d.).
The next sections of this chapter will include a brief historical overview of Canada’s newcomer settlement history, followed by a discussion about the implications for social work practice. The discussions on implications for social work practice emphasize the importance of ensuring accessible and culturally relevant services; a focus on the importance of understanding and embracing cultural diversity; the importance of building trusting relationships; and the issue of newcomer settlement within the context of the Truth and Reconciliation Calls to Action.
The chapter emphasizes that social work practice in rural and northern areas offers an array of practice options for social workers: micro, mezzo, and macro because of the complexity of issues.
Learning Objectives
By the end of this chapter you will have had the opportunity to:
- Engage in critical reflection of newcomer settlement history in rural and northern Canada;
- Build knowledge of the complex, intersecting issues experienced by newcomer settlers in rural and northern areas; and
- Reflect on the implications for social work practice with newcomer settlers, in light of the Truth and Reconciliation Calls to Action (Truth and Reconciliation Commission of Canada, 2015).
Background
Immigrant/newcomer settlement in rural and northern Canada has survived despite the growth of industrialization and urbanization which led to the majority of immigrant settlers heading to larger centres such as Toronto, Vancouver, and Montreal (Patel et al., 2019). Provincial Nominee Programs (PNPs) and other policy and program developments have served to bolster settlement in smaller centres, northern, and rural communities across Canada, thereby increasing the diversity in terms of populations and needs. Newcomer settlement has had different impact on different groups of people and communities.
For Indigenous peoples, immigrant/newcomer settlement meant the loss of lands and long-lasting negative impacts on their food security, health and well-being. More specifically, loss of traditional lands resulted in loss of traditional ways of life and in a reliance on European foods (Hossain & Lamb, 2020; Robidoux & Mason, 2017). The long-term impact has been the emergence of physical and mental health challenges among Indigenous peoples in northern and rural communities (Hossain & Lamb, 2020). Indigenous peoples have continued to organize and engage in various strategies to address the historical impact. More recently, the Truth and Reconciliation Commission’s Calls to Action exposed the history of genocide experienced by Indigenous peoples, and provided a comprehensive list of action items to which Canadians are called to respond (Truth and Reconciliation Commission of Canada, 2015).
While immigration policies resulted in losses for Indigenous peoples, they offered the promise of land and prosperity for settlers, many of whom left countries of origin because of economic and social conditions such as violence, poverty and lack of access to land ownership in those countries (Pedersen, 2004). Describing the evolution of immigration policy, Fleras (2014) summarized it as:
Patterns of immigration to Canada corresponded with the changing requirements of its economy. A pre-First World War concentration on agricultural development and domestication of the West gradually segued into a post-Second World War demand for unskilled labour to extract resources or stimulate industrial growth. More recently, emphasis has shifted towards a reliance on highly skilled immigrants as part of a master plan in transitioning towards a global/knowledge economy. (Reitz, 2003; Simmons, 2010, as cited in Fleras, 2014, p. 6)
Many of Canada’s aggressive immigration strategies developed in the 19th century even though settlers had been arriving long before this. The federal government’s early immigration plan initially aimed at attracting White settlers from Britain and Northern Europe to fill labour market needs. The United States was also seen as a viable source country. The promise of employment in infrastructure development (for example, the rail industry) and in agricultural activity was an early attraction, especially in Western Canada (Friesen, 1987; Shepard, 1997). The emergence of settler clusters in rural communities was often facilitated by word of mouth or chain migration. Canada’s ethnic and cultural diversity continued to grow because of the diversity among these settler populations.
Europeans originating from regions outside of Northern Europe experienced racist and discriminatory policies and practices during the early years of Canada’s immigration outreach (Dobrowolsky, 2017). While these latter populations were not immediately welcomed, Canada eventually opened its doors to them. Consequently, a dominant White settler population emerged in rural Canada, with stories of classism, racism, and discrimination affecting these early settler populations in diverse ways, depending on country of origin. The “Whites Only” and/or Whites preferred policies are evidenced by policies, statements, and actions by a long list of Canadian leaders such as Mackenzie King, Wilfrid Laurier, and Robert Borden. Together, these leaders promoted anti-Black, anti-Asian, and other migration strategies and policies in order to limit or restrict settlement populations (Crawford-Holland, 2020; Dobrowolsky, 2017; Niergarth, 2010; Walker, 1985).
Despite the Whites only and/or preferred policies, non-White populations made their way to Canada’s rural and northern communities, also because of the political, social, and economic conditions of source countries. Non-white settlers who were prepared to accept employment as farm or domestic workers were granted entry (Anwar, 2014; Silvera, 1989). Black Americans travelled from the Southern United States of America (USA) to Oklahoma, and then to Canada hoping to find a welcoming country that would offer land and opportunities for a better life (Crawford-Holland, 2020; Walker, 1985). Instead, they encountered a country where systemic racism was embedded within the cultural and social fabric of host communities. Notwithstanding, there are examples of Black settlers setting up successful farms and homesteads in Prairie rural communities such as Amber Valley in Alberta, Maidstone in Saskatchewan, and Swan River in Manitoba (Irby, 1985; Johnsrude, 2004; Shepard, 1997). Canada’s openly racist policies remained in place until 1967 when new immigration regulations were introduced.
The 1967 Immigration Points System introduced changes within immigration policy by placing emphasis on skills, education, and training rather than on factors such as race, ethnicity, and country of origin during the recruitment or screening stage (Anwar, 2014). This Points System reflected a movement away from a focus on agriculture and rural development towards urban development (Verbeeten, 2007). Canada’s 1988 Multiculturalism Act was designed to move the country even further (Berry, 2013). Nevertheless, evolving policies and legislation did not result in the elimination of systemic racism. For example, while the Points System recognized the skills and backgrounds of applicants, this did not necessarily translate into jobs for all newcomers. Canada recruited the brightest and most gifted from developing countries but did not recognize their credentials and out of country work experience when they actually arrived in Canada. Racialized newcomers were often the victims of these discriminatory policies.
More changes were made when provincial nominee programs started emerging after 1998, leading to new immigrant settlement in smaller centres, rural, and northern communities. Nominee programs have provided opportunities for smaller provincial centres, northern, and rural communities to recruit newcomer settlers from varied social, economic, and cultural backgrounds (Bonikowska et al., 2017). Provinces and communities recruited individuals whom they considered to be best suited for their immediate, often short-term needs. Carter et al. (2010) suggest that provinces were usually able to attract newcomers with lower- level skills and/or with specific skill and trades backgrounds. These settlers might not have qualified under the federal skilled worker program. The Northern and Rural Immigration Pilot and the Agri-Food Pilot pathways were launched in 2019. These pathways have offered further opportunities for welcoming communities to attract newcomers to their locations.
Another significant pathway is the temporary foreign worker program which allows employers to hire temporary foreign workers when there are no Canadians available for the jobs. The program includes a focus on highly skilled professionals, seasonal agricultural workers, and domestic workers. The stories of exploitation and abuse of temporary foreign workers are rampant and have been repeatedly raised (Barnetson et al., 2017; Bryan, 2019; Narushima & Sanchez, 2014; Salami et al., 2015). However, these same workers are often reluctant to rock the boat since their participation in the programs and the resultant income are a lifeline for source countries. Families and communities depend on remittances and workers are reluctant to speak out about poor work conditions.
Finally, communities in rural and northern Canada have experienced periods of economic boom and bust, with accompanying employment, economic, and population growth and decline (Dobson et al., 2014; Marchand, 2012). Newcomer settlers have taken advantage of periods of boom and have also experienced the effects of bust. This is particularly relevant to newcomers who moved to northern communities where mining has been occurring (Coderre-Proulx et al., 2016). The arrival, or parachuting in, of newcomers (including interprovincial and international migration) for employment purposes has had significant impact on local communities. In some situations, companies have made investments into local infrastructure, but this has been inconsistent. A study by the Canadian Research Institute for the Advancement of Women described some of the issues facing northern fly-in and fly-out communities (Leung et al., 2016). Many of these communities do not have year-round road access so often depend on air travel. Accommodation may be temporary or portable, and not appropriate for families who are often based elsewhere. In boom times, the arrival of workers and their families in the hub northern or rural communities that serve the mining sites, has resulted in booming opportunities and business for hotels, restaurants, transportation companies, and stores.
At the same time, boom has had other impacts such as skyrocketing rental and housing prices, and challenges for non-mining companies to find workers because these companies are unable to match the high salaries of the mining companies. Those residents who are not employed directly in the mining sector are disadvantaged by the lower wages and skyrocketing prices. Temporary foreign workers employed in the service sector outside of the mining sector are faced with low wages and often overcrowded accommodations. Some research has identified other issues such as women’s vulnerability to violence and an increase in substance abuse issues. An issue that continues to be raised is the impact of mining on the environment, the impact on women and Indigenous communities in the north, and the extent to which dialogue and genuine consultation has been done to identify the impacts of developments on the lives of Indigenous and northern peoples.
The next section will discuss implications for social work practice. The overall message is that the stories and experiences of newcomer settlement are complex and varied. As such, the aim of the section is to encourage students to explore the diverse opportunities that are available to them to address the needs of newcomers in northern and rural communities.
Implications for Social Work Policy and Practice
Overall, stories of life in northern and rural communities offer accounts of tremendous generosity and hope but also provide insight into the extent to which location away from major centres (place/geography) has posed a variety of challenges for newcomer setters and residents in these communities (Burnett et al., 2020; Kulig & Williams, 2011; Patel et al., 2019; Reid, 2019). These challenges include isolation, and unequal access to affordable public transportation, social services, health, and education resources (particularly specialist services). In addition, systemic racism and discrimination continue to be a major issue in communities across Canada.
Social work with newcomer settlers in rural and northern communities therefore offers an array of possibilities for social work practice: direct social work practice, community development, research, advocacy, education, and social policy. The hope is that social workers will engage in practice to support immigrant/refugee/newcomer settlement in these communities, celebrate the strengths of rural and northern communities, and address the disparities experienced as a result of northern and/or rural living.
As noted earlier, immigrant settlement in northern and rural communities has been driven primarily by economic considerations, and by economic and political developments both within source countries and internally in Canada. Immigration patterns and experiences have also been shaped by the talents/expertise that settlers bring to Canada and by government immigrant selection policies (Bonikowska et al., 2017; Kolbe & Kayran, 2019). The end result for communities is the arrival of newcomers from diverse backgrounds including diverse ethno-cultural, professional, educational, language, and class backgrounds. These are important considerations when striving to understand rural and northern immigrant settlement in Canada. The considerations identified above are particularly significant when working to ensure that settlers are able to (1) create a sense of home in their new locations; (2) have access to job and education opportunities that genuinely recognize and credit the credentials, knowledge, and skills which they bring from other countries; (3) have access to culturally relevant and appropriate supports, resources, and services to enhance their settlement and retention in their new locations; and (4) have a sense of well-being that allows them to flourish. They are also relevant issues for social workers who strive to address issues holistically, and who recognize the layered, multidimensional aspects of issues.
Social workers are therefore challenged to remember that a “one size fits all” will not work for newcomer settlers in rural and northern communities. Newcomers may be highly skilled professionals working in the mining and scientific sectors, and they may also be low skilled workers working in lower skilled agricultural or service sector jobs. They may be highly skilled professionals having left situations of violence and extrema trauma. They may be taxi drivers with professional backgrounds who are working other jobs to support families here in Canada and in countries of origin. Social workers will need to develop the knowledge and skills to learn about and understand these diverse realities. As well, communities will need to engage in ongoing reflection, training, and capacity building in order to ensure they are appropriately responsive to the new populations. As discussed in the following sections, policymakers, advocates, and community workers in rural community will need to constantly review, transform, and develop services and resources to respond to the diverse needs of their new arrivants. Areas of concern and need include availability of resources and infrastructure, understanding and embracing cultural diversity, building trusting relationships, and the issue of social work in rural and northern communities in light of the Truth and Reconciliation Calls to Action.
Availability of Resources and Infrastructure
It is worth emphasizing that studies focusing on the retention of newcomer settlers (those arriving as immigrants and refugees) have consistently noted factors such as access to employment (facilitated by recognition of foreign credential and non-Canadian work experience), education, and cultural communities as strong influencers on decisions to remain in communities, or to relocate (Carter et al., 2010; Krahn et al., 2005). Patel et al. (2019)’s scoping review identified factors such as social inclusion, culturally-appropriate services, gender, and housing as distinct social determinants of health factors relevant to well-being in rural and northern communities. Newcomer status adds another layer to these intersecting factors.
More specifically, in addition to generic health and social services, access to formal settlement services (infrastructure) offering language assessment and training programs, employment readiness programs, and mentorship programs have also been identified (Carter et al., 2010; Krahn et al., 2005). Unfortunately, formal settlement infrastructure has not been consistently available in northern and rural areas. Formal infrastructure, which can be seen as sites offering a level of cultural safety, has provided venues where newcomers can reach out to other newcomers and service providers, access resources and support services, raise issues relevant to their settlement needs, and address some of the isolation that they tend to experience. Infrastructure that includes newcomer information centres provides one-stop centres where newcomer immigrant settlers can begin to learn about what services and resources are available in communities. The Northern and Rural Immigration and the Agri-Food Pilots are programs that are well positioned to fill such gaps since they are expected to ensure the availability of settlement and mentoring opportunities for newcomers (Government of Canada, 2021). Many of these welcoming communities already serve as hubs and outreach centres for those living in small towns, on farms, and in other rural locations. The assumption is that these newcomer gateway projects will expand existing resources.
One area where social work intervention would be useful would be to advocate for the development of infrastructure and services that might be missing. This could include advocating for interpreter services for newcomers who are accessing health and education services. Those social workers interested in macro practice could play a leadership role in bringing together various stakeholders to facilitate discussions and research about the development of such services. Another area would be engaging in direct micro practice within settlement agencies, health care, and the schools that newcomer children would be attending. Various communities now have Settlement Worker in School programs (SW1S) as well as social workers who provide a range of referral, support and mentorship services relevant to newcomer children and their families. Finally, social workers in settlement agencies, health, education, and other sectors may choose to engage in group work practice. This would be particularly useful for women who are survivors of abuse and violence; and would be a site where education about issues of violence and abuse could occur. More than anything else, social workers need to have the relevant and appropriate competencies to work well with newcomer women and their families. The next section explores the wide range of personal values and ways of being that all players---- including newcomers, community residents, community workers, and social workers—bring to communities and the relevance of these to successful settlement of newcomers into rural communities.
Understanding and Embracing Cultural Diversity
Newcomers to Canada have tended to move to larger metropolitan centres. As a result, ethnic and cultural diversity of rural and northern communities has evolved at a slower pace than within larger centres. This has been changing over time because of immigration policies, and also because of the emergence of more employment and business opportunities in rural and northern communities. Nevertheless, newcomers are moving into rural and northern communities whose populations may be tightly knit because of longstanding history and well-established relationships (Herron et al., 2021). The same factors that have positive impacts may also include troublesome elements for these populations. Rural residents may have lived in communities for a long time and cultivated a community culture that is slow to change and accept new ideas and ways of being. This reluctance may be driven by a commitment to preserving what is perceived to be dominant, acceptable traditions and cultures.
Those individuals who do not “fit” into the mainstream may include those who are living in poverty, Indigenous peoples, racialized peoples, and gender diverse peoples. Newcomer settler /immigrant/refugee status adds another intersecting dimension, especially when the country of origin is that of a developing country, is not seen to be adequately “Western”, and where English or French (depending on the location) is not the dominant language. Settlement workers, sponsorship groups, and social workers are faced with the challenge of working together to create communities that are open to embracing diversity, equity, and inclusion. This includes facilitating conversations and activities with messages about how diversity will add richness to existing cultures and communities.
In short, newcomers are coming from diverse cultural backgrounds and are living both positive and challenging realities. A huge challenge is to avoid essentializing cultural identity. Essentialist views of identity view identity as singular, fixed and stereotypically applied without paying attention to diversity within cultures and nationalities (Zilliacus et al., 2017). In other situations, there is a tendency to exoticize people of different cultural backgrounds by an over-emphasis on dance, food, and dress (Zilliacus et al., 2017). Social workers are encouraged to engage in critical reflection of the meaning of cultural diversity in order to arrive at a place where they recognize the multiple, rich, evolving, and complex identities of individual newcomers.
Well-intentioned social workers who fail to acknowledge these complexities, add fuel to existing tendencies to demonize or degrade non-Western cultures. For example, lack of acceptance or understanding of non-Christian cultures may lead to Islamophobia. An assumption that Muslim women wearing head coverings are all living in situations of submission fails to recognize the diversity among Muslim women wearing head coverings. In addition, ignorance about the rich cultural heritage of newcomers from many developing countries may lead to patronizing and paternalistic approaches by settlement workers and sponsorship groups. These issues, while common across different geographies, may be particularly problematic in rural and remote regions. Outcomes of ignorance, assumptions of superiority of one culture and way of being over others, and a drive to maintain the resulting status quo are reflected in racism and gender-based discrimination. These issues may be even more intensely felt in rural and northern communities because of geographic location as well as the size of the communities.
There are multiple, interconnected elements to be addressed when seeking to support newcomers in their new homelands, and particularly in northern and rural communities. At the same time, rural and northern communities have well-established traditions of caring for one another. Social workers and other community workers are encouraged to draw on these positive traditions, and play leadership roles in working in partnership with communities to build awareness of the strengths, contributions and complex realities of newcomers. In addition, it is vital that social workers continue to examine their own biases and assumptions throughout their social work careers in order to be part of a process that has positive outcomes for newcomers in rural and northern communities. These actions will go a long way to build trusting relationships that are central to healthy communities.
Building Trusting Relationships
Several studies and reports have exposed the extent to which xenophobia, racism, gender-based discrimination and lack of cultural safety permeate the fabric of rural and northern Canada; and the extent to which these factors have had extensive negative impact on the well-being of communities (Du Mont & Forte, 2016; Higginbottom et al., 2016; Patel et al., 2019; Tungohan, 2017). Higginbottom and others have described how language barriers compromise accessibility to health services. They have also cited examples of newcomer women not understanding the concept of consent or not having faith in service providers’ respect for confidentiality. They comment that newcomer women have not always been able to develop trust and build relationships with service providers because the sessions and processes, including communication styles, are often too fast paced. This results in service users not always understanding or trusting the proposed plans or interventions.
Social workers and other service providers will need to be continually aware of the need to improve their communication skills. This includes paying attention to the pace at which messages are communicated, ensuring the availability of brochures, pamphlets, and messages in multiple languages, and the availability of interpreters and cultural brokers. Of particular note to younger practitioners is to remember to slow down the pace of their speech, without sounding patronizing.
Social workers have a responsibility to ensure that services are relevant and accessible, and that they are able to provide the kinds of services that newcomers will access. Attending workshops and training opportunities to build competency skills will be helpful in building/enhancing communication competency skills for working with newcomers. Engaging in volunteer activities with newcomers in communities and within agencies will serve to build relationships and create visibility and messages of genuine interest and caring to newcomers. These kinds of initiatives will address the longstanding concerns that newcomers do not access mental health support services, even when there are concerns about the need to respond to histories of trauma and the impact on mental health and well-being.
Newcomers in rural and northern communities ought to have access to resources and services similar to those available to residents of larger, urban centres. Social workers and other health care providers recognize the issues of trauma and the accounts of mental illness experienced by many newcomers. However, they are still not always able to provide care because of varied cultural understandings and interpretations of mental illness, which often result in newcomers not accessing services. Other factors include the lack of familiarity with Western models of mental health services, lack of faith in the ability of service providers to respond to their needs, and the issue of stigma associated with mental health. That is, many of the health care needs experienced in urban centres are also prevalent in rural and northern areas. However, communities are now faced with the additional challenge of ensuring the availability of professionals who have the relevant competency skills to work with these diverse newcomer populations.
Technology plays a role in accommodating some of the disparities resulting from geographic distance away from main centres for all citizens. The COVID-19 pandemic highlighted the role of technology such as tele-health and e-health services, and social media tools particularly in rural and northern communities. It also exposed disparities when residents in rural and northern communities experienced unequal access to these same resources and services because of lack of adequate technology infrastructure (bandwidth as an example), and unequal financial resources to access this infrastructure. These are broad issues with which social workers can also be involved.
The above discussions have focused primarily on the role of communities and social workers in providing a welcoming place to newcomers who are arriving from other countries and settling in Canada’s rural and northern regions. Newcomers continue to arrive in Canada at a time when Canadians are grappling with the histories of exclusion, colonization, trauma, genocide, and violence experienced by Indigenous peoples in their own traditional lands. The next section of this chapter emphasizes that ethical social work practice in rural and northern communities requires that social workers learn about the histories of Indigenous peoples, and engage in practice that is grounded in principles of social justice.
Social Work in Rural and Northern Communities within the Context of the Truth and Reconciliation Calls to Action
One of the points raised in the introduction of this chapter is about Canada’s colonial history with Indigenous peoples. The chapter began by noting the loss of land and culture, and the violence experienced by Indigenous peoples. This final section will draw on the United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP) to discuss the role of social work in rural and northern communities within the context of the Truth and Reconciliation Calls to Action (United Nations, 2008). UNDRIP challenges the doctrine of racism and expresses condemnation for the historic injustices suffered during Canada’s colonial rule. The document names the loss of land and resources and applauds the pathways adopted by Indigenous peoples to organize in order to end all forms of discrimination and oppression. It also calls on states to provide prevention measures and redress in response to the colonial history. That is, UNDRIP makes a strong case for social justice. UNDRIP’s declaration of the inherent rights of Indigenous peoples is well aligned with the Social Work Code of Ethics and particularly well synced with value 1: Respect for Inherent Dignity and Worth of People, value 2: Pursuit of Social Justice, and value 3: Service to Humanity. The door is open to social workers engaged with newcomers in rural and northern communities to work with newcomers so that they are immediately engaged in learning about and reflecting on Canada’s colonial history and about the Truth and Reconciliation Commission’s Calls to Action.
The United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP) raises important questions about settler work in mining and extraction industries in particular. How has engagement with Indigenous peoples taken place? Have impact benefit agreements been developed in partnership with Indigenous peoples? (Amyot et al., 2012; Levac & Manning, 2019; Levac et al., 2016). UNDRIP also raises issues about the impact of all developments on the environment and the importance of proactive, consistent discussion with Indigenous people. That is, social workers have an opportunity to work with newcomer settlers so that they are engaged, as fully as possible, in new ways of being with Indigenous peoples. There should not be delay with these kinds of partnerships, teaching opportunities, and dialogue. Some concrete strategies for social workers include facilitating joint attendance at cultural, educational, and social events hosted by Indigenous peoples and newcomer settlers; development of joint social and community activities to build relationships and learn from one another; and facilitating events with attendees from a broad range of backgrounds, including Indigenous individuals and newcomer settlers.
Conclusion
The issues of newcomer settlement in Canada are complex and forever evolving. The pandemic (2019 and beyond) has added complicating factors since Canadians have been required to pay attention to social distancing, to vaccinations, and to doing everything to keep residents safe. This has created an additional burden on social workers who have traditionally worked hard on building human relationships through personal connecting. It has also created stress for communities where personal contacting has always been important. Clearly, technology and social media have helped to respond to the basic human need of connecting with one another. This chapter noted that the pandemic also exposed that not everyone has equal access to the full benefits of technology. This has certainly been the case for northern and rural communities, and will be an area to which policymakers and scientists will continue to attend. Social workers will also need to respond to concerns that not all older adults are comfortable with the use of technology. When immigrant status and language barriers experienced by newcomers are added to the mix, the concerns become more complicated.
The chapter has challenged social workers to understand and embrace cultural diversity and to avoid essentializing cultures and perpetuating assumptions of the superiority of one culture over another. The chapter recognizes the strengths of rural and northern communities and the different ways in which community is built. This includes the sites where community building and dialogue takes place (for example, seniors’ centres, coffee shops and coffee rows, Legion centres, churches, and Elks Halls). The chapter concludes that social workers have a role to play to build bridges between newcomers, residents, and others connected to these locations.
The chapter identifies problematic issues that are present in communities. These include the experiences of temporary foreign workers whose contributions help to sustain communities, but whose experiences of precarity and exploitation are troublesome. These continue to occur at a time when communities are striving to set themselves up as welcoming communities. The chapter also points to Canada’s longstanding history of racism and to the importance of open discussion focused on unraveling root causes in order to address equity and inclusion.
The United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP), along with the Truth and Reconciliation Calls to Action, together provide documents that social workers doing work with newcomers in rural communities can use to facilitate new ways of building relationships and working with Indigenous peoples and Canadian peoples. The documents can also provide important lessons about how to work with newcomer immigrants so that mistakes made with Indigenous peoples, are not repeated by immigrant settlement agencies.
Finally, this chapter recognizes over and over again, the complexities of issues and circumstances relevant to the lives of newcomer immigrant settlers. The chapter recognizes the multiple, intersecting identities of newcomers, and challenges social work students to dive deeper into these and other complex identities and experiences, for example: newcomers with disabilities, newcomers with diverse sexual orientations and gender identities, and newcomers at various life stages. Of particular note for further reflection is the situation of older racialized diasporic adults. These individuals would have come to Canada as immigrants or refugees but are now Canadian citizens. They may have lived as minorities in northern and rural communities for decades and continue to have strong connections to ancestral countries of origin. That is, doing solid, ethical practice with newcomers in Canada’s rural and northern communities calls on social workers to push themselves to be open to the forever changing and complex realities and contexts of these arrivants, settlers, and communities.
Judy White is a Black woman who was born and raised in Trinidad and Tobago. Having been raised in a country with a long colonial history, Judy understands that independence did not lead to an immediate decolonial status. As such Judy’s academic, practice, and community work has been informed by critical race and Black feminist theoretical frameworks; and by a deep commitment to decolonization and social justice. Most of Judy’s early direct social work practice was carried out in rural Saskatchewan.
Activities and Assignments
- Students are encouraged to locate a settlement agency or immigrant gateway agency in a rural or northern region and discuss the services that are provided. What language supports are available? What services are offered? What is the geographic reach of the agency? What is the general profile of the newcomers they are seeing in their agency? What is the educational background of the workers? How did the community come to have a settlement agency?
- Choose a rural or northern community. What have been the newcomer settler trends over the past 5 years? What might be some of the emerging social issues? What have been the responses? What gaps in services exist? What have been the contributions of the newcomer settlers?
- Students are invited to review the list of communities participating in the Rural and Northern Immigration Pilot and the Agri-Food Pilot. Students are asked to choose two (2) communities to focus on. They are to develop a brief profile of these communities, identify the kinds of newcomer populations that are arriving, and highlight the potential community services that might be required.
References
Amyot, S., Stinson, J., Stienstra, D., & Chansonneuve, D. (2012). Women, economic development & restructuring in Thompson. Canadian Research for the Advancement of Women. https://www.criaw-icref.ca/wp-content/uploads/2021/04/Women-Economic-Development-and-Restructuring-in-Thompson.pdf
Anwar, A. (2014). Canadian immigration policy: Micro and macro issues with the points based assessment system. Canadian Ethnic Studies, 46(1), 169-179.
Barnetson, M., Barnetson, B., & McDonald, S. A. (2017). Farm workers in western Canada: Injustices and activism. University of Alberta Press.
Berry, J. W. (2013). Research on multiculturalism in Canada. International Journal of Intercultural Relations, 37(6), 663-675.
Bonikowska, A., Hou, F., & Picot, G. (2017). New immigrants seeking new places: The role of policy changes in the regional distribution of new immigrants to Canada. Growth and Change, 48(1), 174-190.
Bryan, C. (2019). Labour, population, and precarity: Temporary foreign workers transition to permanent residency in rural Manitoba. Studies in Political Economy, 100(3), 252-269.
Burnett, K., Sanders, C., Halperin, D., & Halperin, S. (2020). Indigenous peoples, settler colonialism, and access to health care in rural and northern Ontario. Health & Place, 66, 102445.
Carter, T., Pandey, M., & Townsend, J. (2010). The Manitoba provincial nominee program: Attraction, integration and retention of immigrants (IRPP Study). Institute for Research on Public Policy.
Coderre-Proulx, M., Campbell, B., & Issiaka Mandé, I. (2016). International migrant workers in the mining sector. International Labour Organization.
Crawford-Holland, S. (2020). The birth of a nation in Canada: Black protest and white denialism across Canada's colour lines. Film History, 32(4), 1-32.
Dobrowolsky, A. (2017). Bad versus big Canada: State imaginaries of immigration and citizenship. Studies in Political Economy, 98(2), 197-222.
Dobson, S., Lemphers, N., & Guilbeault, S. (2014). Booms, busts and bitumen: The economic implications of Canadian oilsands development. The Pembina Institute and Équiterre.
Du Mont, J., & Forte, T. (2016). Perceived discrimination and self-rated health in Canada: An exploratory study. BMC Public Health, 16(1), 742.
Fleras, A. (2014). Immigration Canada: Evolving realities and emerging challenges in a postnational world. UBC Press.
Friesen, G. (1987). The Canadian prairies: A history. University of Toronto Press.
Government of Canada. (2021). Immigrate to Canada. https://www.canada.ca/en/immigration-refugees-citizenship/services/immigrate-canada.html
Government of Canada. (n.d.). Immigrate through the economic mobility pathways pilot: Who is eligible. https://www.canada.ca/en/immigration-refugees-citizenship/services/refugees/economic-mobility-pathways-pilot/immigrate/eligibility.html
Herron, R., Newall, N., Lawrence, B., Ramsey, D., Waddell, C., & Dauphinais, J. (2021). Conversations in times of isolation: Exploring rural-dwelling older adults' experiences of isolation and loneliness during the COVID-19 pandemic in Manitoba, Canada. International Journal of Environmental Research and Public Health, 18(6), 3028.
Higginbottom, G., Safipour, J., Yohani, S., O'Brien, B., Mumtaz, Z., Paton, P., & Barolia, R. (2016). An ethnographic investigation of the maternity healthcare experience of immigrants in rural and urban Alberta, Canada. BMC Pregnancy and Childbirth, 16(1), 20.
Hossain, B., & Lamb, L. (2020). Cultural attachment and wellbeing among Canada’s Indigenous people: A rural urban divide. Journal of Happiness Studies, 21(4), 1303-1324.
Irby, C. C. (1985). Black settlers at Amber Valley, Alberta. The Western Journal of Black Studies, 9(1), 2.
Johnsrude, L. (2004, March 7). Blacks celebrate role in Alberta's settlement: About 1,000 U.S. migrants came in early 1900s. Edmonton Journal.
Johnston, A. (2020). Defining rural teaching hospitals in Canada: Developing and testing a new definition. Canadian Journal of Rural Medicine, 25(4), 1.
Kolbe, M., & Kayran, E. N. (2019). The limits of skill-selective immigration policies. Journal of European Social Policy, 29(4), 478 – 497.
Krahn, H., Derwing, T. M., & Abu-Laban, B. (2005). The retention of newcomers in second- and third- tier Canadian cities. The International Migration Review, 39(4), 872-894.
Kulig, J. C., & Williams, M. (2011). Health in rural Canada. UBC Press.
Laurin, F., Pronovost, S., & Carrier, M. (2020). The end of the urban-rural dichotomy? Towards a new regional typology for SME performance. Journal of Rural Studies, 80, 53-75.
Leung, W., Wilcox, C., White, J., Careen, N., Hutchison, C., & Lake, V. (2016). Fly-in and fly-out communities in Northern Canada. Canadian Research Institute for the Advancement of Women.
Levac, L., & Manning, S. (2019). The importance of Indigenous and Northern women’s experiences and knowledges in impact assessments. Canadian Research Institute for the Advancement of women. https://www.criaw-icref.ca/wp-content/uploads/2021/04/The-Importance-of-Indigenous-and-Northern-Womens-Experiences-and-Knowledges-in-Impact-Assessments.pdf
Levac, L., Manning, S., Stienstra, D., Baikie, G., & Stinson, J. (2016). What do gender and diversity have to do with it? Responding to the community impacts of Canada’s resource development agenda. Canadian Research Institute for the Advancement of women. https://www.criaw-icref.ca/wp-content/uploads/2021/04/What-do-gender-and-diversity-have-to-do-with-it.pdf
Marchand, J. (2012). Local labor market impacts of energy boom-bust-boom in Western Canada. Journal of Urban Economics, 71(1), 165-174.
Narushima, M., & Sanchez, A. (2014). Employers' paradoxical views about temporary foreign migrant workers' health: A qualitative study in rural farms in southern Ontario. International Journal for Equity in Health, 13(1), 65.
Niergarth, K. (2010). ‘This continent must belong to the white races’: William Lyon Mackenzie King, Canadian diplomacy and immigration law, 1908. The International History Review, 32(4), 599-617.
Patel, A., Dean, J., Edge, S., Wilson, K., & Ghassemi, E. (2019). Double burden of rural migration in Canada? Considering the social determinants of health related to immigrant settlement outside the cosmopolis. International Journal of Environmental Research and Public Health, 16(5), 678. https://res.mdpi.com/ijerph/ijerph-16-00678/article_deploy/ijerph-16-00678.pdf
Pedersen, M. (2004). "Wherever two or three are gathered": A study of the Finnish settlement at New Finland, Saskatchewan, 1888-1945 [Master’s thesis, University of Regina]. ProQuest Dissertations and Theses Global.
Reid, S. (2019). The rural determinants of health: Using critical realism as a theoretical framework. Rural and remote health, 19, 5184.
Robidoux, M., & Mason, C. (2017). Introduction. In M. Robidoux & C. Mason (Eds.), A land not forgotten: Indigenous food security and land-based practices in Northern Ontario (pp. 1-15). University of Manitoba Press.
Salami, B., Meharali, S., & Salami, A. (2015). The health of temporary foreign workers in Canada. Canadian Journal of Public Health, 106(8), E546-E554.
Shepard, B. R. (1997). Deemed unsuitable: Blacks from Oklahoma move to the Canadian prairies in search of equality in the early 20th century only to find racism in their new home. Umbrella Press.
Silvera, M. (1989). Silenced: Caribbean domestic workers talk with Makeda Silvera. Sister Vision, Black Women and Women of Colour Press. (Original work published in 1983)
Truth and Reconciliation Commission of Canada. (2015). Truth and Reconciliation Commission of Canada: Calls to action.
Tungohan, E. (2017). From encountering confederate flags to finding refuge in spaces of solidarity: Filipino temporary foreign workers' experiences of the public in Alberta. Space & Polity, 21(1), 11-26.
United Nations. (2008). The United Nations Declaration on the Rights of Indigenous Peoples. Office of the High Commission for Human Rights.
Verbeeten, D. (2007). The past and future of immigration to Canada. Journal of International Migration and Integration, 8(1), 1-10.
Walker, J. (1985). Racial discrimination in Canada: The Black Experience.
Zilliacus, H., Paulsrud, B., & Holm, G. (2017). Essentializing vs. non-essentializing students' cultural identities: Curricular discourses in Finland and Sweden. Journal of Multicultural Discourses, 12(2), 166-180.
This chapter provides an overview of social work practice focused on the delivery of mental health services in rural, remote, and northern communities. As social workers, we know that the prevalence, scope, and range of mental health issues in locations outside of urban centres is significant, and has an impact on the lives of individuals, families and communities. We also know that populations living in these communities don’t always have adequate and necessary access to mental health services and supports. In efforts to fill existing gaps in mental health services, social workers living and practicing outside of urban centres are required to work collaboratively and creatively, while utilizing generalist social work practice skills. Increasingly, mental health issues are a growing public health concern in Canada, with mental illness now identified as one of the leading causes of disability (Chen et al., 2020).
This chapter will highlight the characteristics of rural, remote and northern communities that affect mental health service delivery from a social work perspective; it also discusses select mental health-related issues. Attitudes and beliefs that result in stigma related to mental illness, and towards those experiencing mental health challenges, will also be explored.
Learning Objectives
By the end of this chapter you will have had the opportunity to:
- Understand the scope of practice of social workers providing mental health support services in rural, remote and northern settings.
- Describe factors influencing mental health and addictions outside of urban settings.
- Identify common types of mental health concerns found in rural, remote, and northern settings.
- Understand the barriers and enablers for social workers at the micro-, mezzo- and macro-levels of mental health service provision in rural, remote, and northern settings.
- Recognize how the stigma surrounding mental illness affects service access in locations outside of urban settings, and to identify strategies to reduce that stigma.
What is Mental Health?
The World Health Organization (2021) stresses the importance of understanding mental health as not just the absence of mental illness, but as a concept that applies to everyone under a range of circumstances. The World Health Organization [WHO] defines mental health as a state of well-being in which the individual realizes their own abilities, can cope with regular stresses of life, can work productively, and is able to make a contribution to their community (2021). The Canadian Mental Health Association [CMHA] describes mental illness as a disturbance in thoughts, feelings, and perceptions that is severe enough to affect everyday functioning. Some examples of mental illnesses are anxiety disorders, schizophrenia, and mood disorders such as major depressive disorder and bipolar disorder. Substance misuse is often linked to poor mental health or mental illness (CMHA, 2021). Internationally, and in most jurisdictions across Canada, supports and services are often offered to address both mental health- and addictions-related issues. In the literature, and in practice, mental illness is sometimes referred to as: mental conditions, mental health issues, mental health difficulties, psychological disorders, and challenges to mental health (Baxter et al., 2022; Chen et al., 2020; Lister et al., 2021).
The Mental Health Continuum Model
Within mental health service delivery, the mental health continuum [MHC] model refers to a specific model that has been developed to help with understanding mental health that incorporates a self-help tool. This model is used to:
- Identify the underlying causes of impairment in daily-life functioning;
- Gather information about mental health of individuals over time;
- Indicate when it would be ideal to seek professional assistance for restoring balance in mental health; and
- Learn how to recognize symptoms of psychological disorders (Chowdhury, 2021).
Originally developed by the Canadian Armed Forces [CAF], the MHC model describes four main states of mental health a person could possibly experience. The model is presented as a continuum, which means that a person can move back and forth along the continuum scale and can also land somewhere between the four main areas at any given time (Chen et al., 2020; NSCAD, 2021).
Figure 1
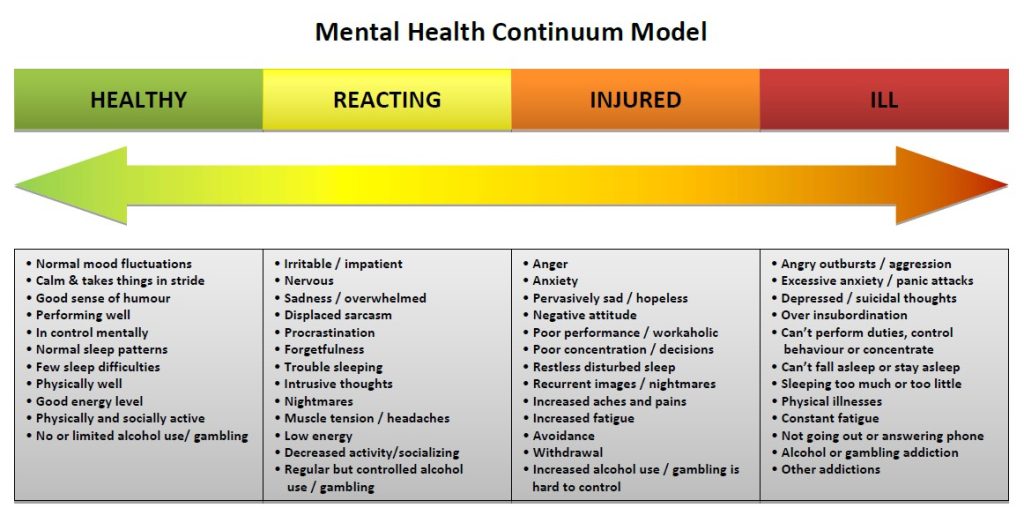
In a more general sense, the mental health continuum refers to a range of mental wellbeing with mental health and mental illness at the two extreme ends. Depending upon the circumstances of an individual at any given point in time, he/she/they can be situated at one point of the continuum but can actually shift position as their situation improves or deteriorates, which is seen as being an effective way to interpret mental health (Allport, 1937; Chen et al., 2020). Consistent throughout the literature is the acknowledgement that there is a place for everyone on the mental health continuum (Chen et al., 2020; Chowdhury, 2021), and that this approach can potentially reduce stigma due to the idea that everyone fits in. The model is intended to serve as a self-reflection and self-monitoring tool, with colours indicating the level of severity of illness. By incorporating colours, the intention is to further reduce stigma by limiting use of jargon and reducing the potential impact of diagnostic labels (Chen et al., 2020). The MHC model has been adopted widely as a tool to promote mental health in various settings and contexts in Canada and internationally (Chen et al., 2020; Franken et al., 2018). The mental health continuum short form [MHC-SF] has been validated in nonclinical samples and incorporated in various countries and cultures (Franken et al., 2018).
Social Workers and the Mental Health Continuum Model
An approach to practice that incorporates the MHC model can be helpful for social workers, regardless of practice setting. However, especially in rural, remote, and northern communities, this model can help social work practitioners to recognize specific behavioral patterns in clients that may need attention and allow them to suggest ways of dealing with service needs in creative ways. Creative approaches and out-of-the-box thinking can be helpful in settings that lack a comprehensive range of formal mental health supports.
For practicing social workers, this model can also offer helpful information to consider as they strive to maintain their own mental health and wellness by serving as a practical and reliable tool for social workers to identify their own sources of personal and professional stress by:
- Understanding how to identify symptoms of mental illness in oneself and others;
- Encouraging the growth and maintenance of a healthy mindset that can assist in overcoming distress and create positive movement on the continuum; and
- Learning how to deal with psychological and emotional crises effectively while not allowing one’s well-being to be jeopardized (Chowdhury, 2021).
Generalist Social Work Practice in Mental Health Service Delivery
Undergraduate social work programs across Canada and North America focus on a generalist approach to social work practice (Weshues et al., 2001). This approach equips social workers with information on the basic concepts in social work, as well as a range of skills and a level of awareness that prepares them for a variety of social work roles in a range of settings. By focusing on generalist practice, students are introduced to ideas that include the promotion of well-being and the application of preventative and intervention methods to address social problems at individual (micro), group (mezzo), and community (macro) levels (Weshues et al., 2001). Although these levels are often spoken of as distinct, they actually occur in tandem and are linked to, and constantly influence, one another.
Rural, remote and northern locations offer unique opportunities for practicing social workers. In fact, many new social workers seek employment in these settings in order to gain practical experience in a relatively short period of time (Schmidt, 2008). Social workers in urban settings will tend to work in areas of practice considered to be more focused and specialized, whereas settings outside of urban areas require the social worker to engage in a number of areas of practice simultaneously. These areas of practice may include child protection services, addictions, mental health, income support, community development, and policy.
Mental Health Enablers and Barriers outside of Urban Settings
As discussed previously in this book, individuals who live outside of urban centres face unique factors that impact directly upon everyday life. While the quality of life in rural, remote and northern communities is idyllic in many ways, and is often sought after, the challenges associated with living outside of large centres can also affect that quality of life in negative ways – especially in relation to mental health. These negative effects include:
- Less comprehensive, available, and accessible support services,
- Transportation limitations due to geographic accessibility,
- Fragmented continuity of care,
- Difficulties with workforce recruitment and retention,
- Lack of access to affordable housing, and
- Limited access to population-based funding (CMHA Ontario, 2009).
In this context, a barrier to access is understood as any process or intervention by which access to mental health supports is impeded. Enablers are defined as any process or intervention by which access to mental health services and wellbeing is facilitated (Baxter et al., 2022; Lister et al., 2021). Figure 2 provides an overview of enablers and barriers to accessing mental health supports in rural, remote, and northern communities.
Figure 2
Enablers and Barriers to Mental Health Support Availability outside of Urban Settings
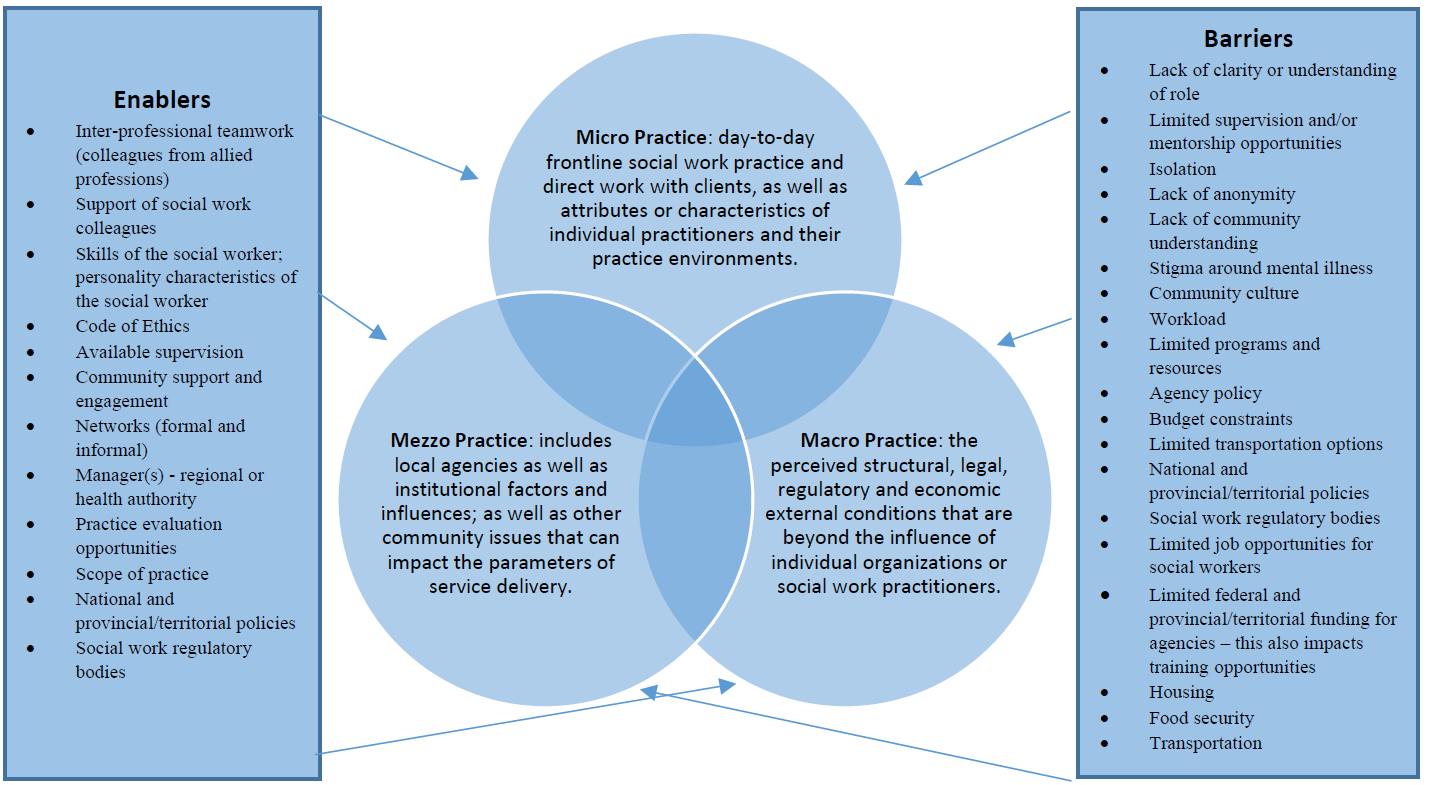
Rural, remote, and northern communities are not homogenous. The populations of people who live in these communities are diverse and represent distinct cultures, ethnicities, ages, and backgrounds. Despite this diversity, most individuals seeking supports and services for mental illness experience widespread stigma regardless of their backgrounds (Friesen, 2019; MacLeod et al., 2022).
Mental Health Issues and Stigma
The concept of stigma has been well-researched over the past 6 decades and has led to the conceptualization of stigma as a social construct. Dudley (2000) defined stigma as “stereotypes or negative views attributed to a person or groups of people when their characteristics or behaviors are viewed as different from, or inferior to, societal norms” (p. 449). These views may focus on what are seen to be mental, physical, or social deficiencies (CMHA Ontario, 2022). Stigma differs from discrimination, which is viewed as unfair treatment due to a person’s identity. This identity can include race, ancestry, place of origin, colour, ethnic origin, citizenship, creed, sex, sexual orientation, gender identity, gender expression, age, marital status, family status or disability, including mental disorder (CMHA Ontario, 2022). In other words, stigma is the negative stereotype, and discrimination is the behaviour that results from this negative stereotype.
It is important to note that, because stigma is a social construct, it changes over time. What was stigmatized in the past may not be stigmatized today, or has changed in terms of how it is expressed at the micro-, mezzo- and macro-levels. This change often will occur as a shifting between the three levels. Goffman (1963) referred to this as the “process of devaluation” (p. 3), which can dehumanize anything or anyone that sits outside the lines of what the community believes to be acceptable. This process can create an “us versus them” scenario that is founded in difference, stereotypes, and misinformation; it can result in fear leading to unfair treatment of individuals. In a rural or remote community, this discrimination can be devastating, as an already small social network can become yet smaller, or even non-existent.
Stigma related to mental illness and mental health issues can have detrimental consequences. The World Health Organization [WHO] (2001) has suggested that stigma is one of the largest barriers to mental illness treatment engagement, despite the fact that treatment has been shown to be effective. Due to stigmatization, people may delay seeking help, may exit treatment prematurely, or may completely avoid seeking services. These realities will often increase psychological distress and when individuals can no longer wait due to an increase in symptoms, the level of distress is significantly greater. Stigma can impact social activities for individuals experiencing mental illness, along with education, housing, and employment; the result is often social isolation. Herek (2002) stated: “stigma and discrimination are the enemies of public health” (p. 604). Stigma in the rural and remote areas of Canada can be further compromised by a shortage of services in the areas of mental health and addictions, and difficulty in accessing those services. Stigma at the micro-, mezzo- and macro-levels, in conjunction with a lack of formal supports, can leave people in a very precarious position.
Social workers work with a variety of complex cases that require a thoughtful approach. Working in rural and remote areas with under-served populations requires the social worker to have a sophisticated level of knowledge and understanding of mental health and mental illness, as well as ethical fortitude. Further, a knowledge base of the current and historical culture of the geographic region in which they are practicing is critically important. No two communities are the same and each will have distinct enablers and protective factors, as well as specific barriers and factors that may put people at greater risk. An insular community may have a variety of protective and enabling factors, but someone who is marginalized within that community may also feel like an outsider. This experience will undoubtedly affect that individual’s mental health. Social workers working in rural and remote communities have a unique opportunity to influence efforts to de-stigmatize mental illness. They will work with individuals and their families and can mitigate stigma at the micro- and mezzo-levels. For example, involving the family will support the individual with mental illness, and help the family to understand conditions impacting mental health; this can re-build the family structure and support system. On a macro-level, the social worker will have opportunities to support educational efforts to de-stigmatize mental illness and advocate for local and regional changes. They can advocate for policy change, and ensure that mental health policy is being developed at the same time and rate as health policy. Through the nature of their generalist practice approaches, social workers will also be networking with various agencies and can be an agent of change to support community-wide mental health and wellness initiatives.
A social worker working in mental health services requires the ability to self-reflect about their own stereotypes, beliefs and prejudices. It is also important to acknowledge that we, the community in which we serve, as well as the person in need; all have known and unknown attitudes about what they are coming to discuss. We must create a space where these attitudes and beliefs can be explored and tested, in order to determine their impact on services.
Areas of Practice in Mental Health Services
As discussed throughout this book, a social worker engaging in practice outside of urban settings will have many opportunities to work with a range of individuals from diverse backgrounds. These individuals will seek support services from social workers in order to deal with many aspects of mental health and mental illness. This section will focus on five select areas of social work practice specific to mental health in rural and remote settings: suicide prevention and intervention, substance use and addictions, chronic mental illness, maternal mental health, and violence.
Suicide Prevention and Intervention
In Canada, suicide is identified as the ninth leading cause of death among the general population. However, for individuals between the ages of 15 and 34, suicide is the second leading cause of death (MHCC, 2022b). In first world countries, men are three times more likely than women to die by suicide (WHO, 2017). Lesbian, gay, bisexual, transgender, queer/questioning and other sexual and gender minority (2SLGBTQ+) youth have also been consistently identified as having an elevated risk for suicide (Wang et al., 2021).
The Mental Health Commission of Canada (2022b) reports that alcohol abuse is the second most common mental health problem identified in people who die by suicide, and one in four deaths by suicide are completed by those who abused alcohol. Suicide rates are also higher in rural areas as compared to urban areas (Creighton et al., 2017; Frederick, 2020; Reccord et al., 2021). The rates of suicide in Canada are consistent with suicide rates in other first world countries that experience similarities in terms of poverty levels, aging populations, lack of employment opportunities, and out-migration to urban centres (Cleary, 2012).
Suicide has had a profound impact on communities that are predominantly First Nations, Métis and Inuit. In fact, the suicide rates among First Nations and Métis adults have been reported to be twice as high as among non-Indigenous adults (Park et al., 2015). The rates of suicide in Northern Saskatchewan are very high, and suicide is identified as the leading cause of death for people aged between 10 years to 40 years (Irvine & Quinn, 2017). Suicide intervention approaches need to be culturally responsive in areas that have a higher First Nation, Métis and Inuit population; where the impacts of colonization and inter-generational trauma are the predominant underlying factors impacting suicide rates.
Suicide prevention strategies should be targeted to the local demographics and culture in rural and remote communities, and designed by local stakeholders with a focus on community needs and assets. Social workers can play an important role in suicide prevention, education, and intervention.
Suicide in in rural and remote areas is of significant concern, yet populations impacted by suicide continue to be overlooked and underserved at all three levels of intervention (micro, mezzo, and macro). A review of the literature by Hirsch and Cukrowicz (2014) identified that successful interventions require a thoughtful approach which focuses on the geographic location, social belief systems, and determinants of health that impact suicide. It is also important to recognize the effects of poverty and lack of employment opportunities, as well as the importance of creating literacy around mental wellness and building trauma-informed communities.
As social workers, we have to pay attention to social, cultural, and economic-specific strengths and adversities of communities, as well as social and cultural norms. Every rural or remote community will have its own nuances about what is stigmatizing, its own history within Canada, and its own trauma legacy.
Substance Use and Addictions
Addictions can affect anyone. The Canadian Mental Health Association estimates that approximately 21% of the Canadian population (about 6 million people) will meet the criteria for addiction at some point in their lifetime (CMHA, 2022). Alcohol is identified as the most common drug used by Canadians, and those living in rural and remote areas of the country were more likely to report heavy drinking compared to those living in urban areas (CCSA, 2019; Statistics Canada, 2019).
The American Society of Addiction Medicine (2019) defines addiction as “a treatable, chronic medical disease involving complex interactions among brain circuits, genetics, the environment, and an individual’s life experiences”. The topic of addictions is vast as it includes the abuse of illegal substances, the misuse of legal substances, as well as compulsive behaviors involving gambling, internet/gaming, and sex. As social workers, it is important to be aware of language and how that language is used in this area of practice. In the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders [DSM-5] (APA, 2021), revisions were made to include Substance-Related and Addictive Disorders with substantive changes to the disorders grouped there, plus changes to the criteria of certain conditions. The DSM-5 explains that the essential feature of a substance use disorder is that it includes a cluster of cognitive, behavioral, and physiological symptoms highlighting that with this disorder, the individual continues using the substance despite significant substance-related problems (APA, 2021). In other words, people with addictions use substances or engage in behaviors that become compulsive and often continue the behaviors despite harmful consequences.
Understanding the complexity of addiction is essential for social workers and those working to support individuals with addictions; Gabor Mate (2011) explains that addiction is more than a disease or human choice, it is a response to human suffering. Using substances may provide the person temporary relief from emotional and physical pain, however it can exacerbate the problem and have harmful impacts on one’s health, relationships, work/responsibilities, finances, and may lead to legal problems.
The misuse of alcohol and drugs is influenced by individual, cultural and social factors which can serve as protective and/or risk factors (enablers and barriers). These factors need to be considered when working with individuals and families as part of preventative programming, intervention/treatments and rehabilitation processes. For social workers working in rural and remote areas with people and communities experiencing addiction, consideration of these factors is essential to the working relationship and change process. First, the rural and remote location must be acknowledged and considered, as these places throughout Canada do not have the same access and availability of services as do urban centres. This can be challenging for individuals and families experiencing concerns with mental health and substance use as it may require additional time and financial resources in order to connect with supports; all which can further complicate one’s physical, social and mental wellbeing.
Telehealth services and online programming are often options that can be beneficial for individuals and families living in rural and remote communities, as these options create possibilities for people to connect with informal and formal supports in order to address physical health concerns, as well as mental health concerns. An example of services being utilized in this way can be found in remotely delivered Alcoholics Anonymous or Narcotics Anonymous group meetings. Online meetings allow people more options to attend virtual gatherings that support their schedule, can reduce the need to travel long distances, and also can provide greater anonymity. Although this modality of service may increase accessibility for some, it is not always possible for others as this approach requires internet access, computer literacy skills and a safe and quiet space to connect. Understanding how these factors can be barriers is essential to the helping process.
Individuals misusing substances can be at different stages in their use and readiness for change. A harm reduction approach includes strategies to reduce individual harm through managed consumption and overdose prevention sites. This approach, which was initially developed in the 1980s, recognizes the individual and meets them “where they are at” to help reduce harm, address basic needs, and increase safety and wellness. This approach to service delivery also increases engagement of clients, and supports willingness to change. Harm reduction and social work share common values and approaches, not the least of which is recognizing the client (service-user) as expert, and using strengths-based efforts to build collaborative working alliances (Vakharia & Little, 2017).
Navigating the system to help support individuals with substance use disorders can be especially challenging in rural and remote locations, due to limited outpatient and inpatient services and waitlists. It is important for social workers to understand how social and health determinants contribute to risk, to the treatment of substance misuse, as well as overall wellbeing.
As discussed earlier, individuals living in rural and northern locations report high levels of excessive use of alcohol. Higher rates of driving while impaired is also common. In recent years, opioid use has emerged as a crisis across Canada, and this issue is especially difficult to address in rural and northern communities. These two types of addictions will be discussed further below, as will the issue of impaired driving.
Alcohol
Accessibility and availability of resources for alcohol abuse prevention, intervention and recovery are influenced by social and cultural factors. Poor socio-economic conditions found in many rural communities is correlated with higher levels of alcohol consumption, psychosocial stress, and decreased physical activity and preventive service use (Smith et al., 2019). The limited resources available create an additional challenge when trying to arrange services that are appropriate and meet the individual’s needs. Rural physicians show an awareness and concern for alcohol consumption in their communities, but they also report difficulties in accessing resources to refer patients for substance use treatment (Slaunwhite & MacDonald, 2015).
Communities with smaller populations and/or communities that are located in isolated areas can create more familiarity for individuals. This factor can be understood as both an enabler and as a barrier when it comes to seeking support services. Familiarity may bring people a sense of belonging and support, yet it can also be isolating for those who don’t fit the identified community norms and expectations. The lack of anonymity can prevent individuals and families from seeking help due to shame and stigma. Stigma continues to be a factor that potentially isolates people experiencing difficulties with substance use.
It may be helpful for social workers to consider a social-ecological perspective for explaining influences on alcohol use. Individual-level factors that influence alcohol use are found within home, work, and school environments, which are located within the larger community. Macro-level factors, such as exposure to advertising, may influence family and peer network attitudes and norms, which ultimately impact individual attitudes and behaviors. Social work focuses on the person within their environment and recognizes the importance of family, community, culture, legal, social, spiritual, and economic influences that impact well-being of individuals, families, groups, and communities.
Opioids
There is an opioid crisis affecting communities across Canada (Pijl et al., 2022). This crisis is affecting individuals, families, and communities, often resulting in long term health issues like HIV and hepatitis, possible overdose, and death.
Jones and Quinn (2021) illustrate the impact of remote geography on clinical decisions, adequate medication supply, and the importance of engaging pharmacy and nursing colleagues in delivering addictions care specific to the use of opioids. National practice guidelines for opioid use disorder recommend buprenorphine–naloxone as a first‑line treatment. In rural areas, medications that can be administered on a monthly basis, like buprenorphine and/or naltrexone formulations, might be particularly effective since distance and transportation can present barriers to daily-dose treatment approaches (NIDA, 2021). Clinical practice guidelines state that methadone maintenance therapy (MMT) is the standard of care for treating patients with opioid dependence. Methadone maintenance therapy is a substitution/maintenance treatment model whereby methadone is administered in a structured treatment environment to reduce or eliminate the uncontrolled use of illicit opioids (NIDA, 2021).
Impaired Driving
Research has shown that rates of impaired driving tend to be about twice as high in rural areas as compared to urban areas (Perreault, 2019). For the purpose of this discussion, impaired driving refers to driving while under the influence of alcohol, cannabis, or other mind-altering substances. Greene et al. (2018) found that these rates were often higher in younger age groups and identified specific factors that contribute to those higher rates: social context (peer pressure and parental modeling), rural cultural values (independence, stoicism, and social cohesion), as well as the realities of the legal and physical environment (minimal police presence, sparse population, and no alternative transportation). Since 2018 when Canada became the second country to legalize non-medical cannabis, emerging research has confirmed that driving under the influence of cannabis is an increasingly prevalent road safety issue (Brands et al., 2021). As discussed earlier, higher rates of cannabis and alcohol use are also linked to increased suicidal ideation in young people. Suicidal ideation, or suicidal thoughts, means having thoughts or ideas about the possibility of ending one's own life.
Social workers practicing outside of large urban centres play a key role in working with individuals with substance use and co-occurring disorders, as well as their families and communities. As such, knowledge about substances, behavioral indicators of substance use, relevant assessment tools, and knowledge about available and accessible treatment and support options is essential.
Chronic Mental Illness
Long-term and chronic mental illness is multi-faceted and complex, requiring a coordination of support and collaboration at all three levels of social work practice (micro, mezzo and macro) beginning when the individual seeks ongoing support, and continuing as they enter into the recovery and long-term support process. Most often in the literature, those with chronic mental illness are identified as individuals with Serious Mental Illness (SMI) (Steele et al., 2014), and this is the term that will be used in this discussion. Individuals with SMI fall at the extreme right side of the mental health continuum and may require a greater level of tertiary care in order to stabilize their mental illness and avoid further deterioration. Those with SMI usually require long-term medication and support, and this can include schizophrenia and schizophrenic‐like disorders, but can also refer to any reoccurring mental illness that produces serious functional impairment and interferes with the person’s quality of life including psychosis and bipolar disorders (Steele et al., 2014). Individuals with SMI typically experience gaps in services and these gaps are more pronounced in rural and remote locations that lack community resources and in-patient capacity.
Individuals with SMI tend to socially isolate themselves and this can have compounding effects on the course of their recovery. A supportive and resourced community can have significant and positive influence on the lives of people living with SMI. Protective factors increase when the social capital of the community is more robust. Social capital includes friends, social norms, networks of support and employment opportunities for the individual with Serious Mental Illness in the community (Dykxhoorn et al., 2019), and can play an important role in the person’s overall mental health and physical wellbeing. Social capital also includes the infrastructure of a community such as parks, libraries and other pro-social activities like volunteering opportunities. In their research, Kitchen et al. (2012) found a very strong association between health (mental health in particular) and a sense of belonging, especially in rural areas of Canada.
Peer support can have a positive impact on the person with SMI, as well as the family who may struggle with their own perceptions of mental illness. Peer support can include group activities, mentoring, and a system of mutual giving and receiving where individuals with SMI can offer hope, companionship, and encouragement to others facing similar challenges (Naslund et al., 2014). Peer support lays primarily in the mezzo-level of support provided by social workers, and can have a significant impact on the micro-level as the social capital increases and the person’s sense of inclusion and community belonging also increase. Individuals with SMI often turn to social media to seek information and create communities to share their experience, and to obtain information from others with a similar diagnosis. This network building can significantly reduce personal and social stigma and normalize experiences as they increase insight about their diagnosis, develop on online community where potentially none exists in their home community, and gain support from others in similar circumstances including gender, age, culture and other demographics that may be important to the individual. However, vulnerability is a potential risk that needs to be considered when entering the online platform.
Individuals with Serious Mental Illness represent 30% to 40% of the homeless population and as many as 25% of those same individuals have a substance dependence (Kirby & Keon, 2006). Although rural and remote homelessness in Canada remains a hidden issue, there is mounting evidence that homelessness is as prevalent in rural communities as it is in urban settings (NAERRH, 2021). As the individual with SMI moves between recovery and maintenance, the importance of housing in the stabilization of psychiatric symptoms is highlighted as a significant factor in their recovery. Stable housing is especially important for social workers to keep in mind when working in rural and remote locations where the interplay between the mezzo- and macro-levels can have a significant impact on the quality of life of the individual. This issue highlights the importance of developing a coordinated and collaborative approach encompassing all three levels of support and intervention (micro, mezzo, and macro). Social workers can provide individual support, as well as sessions for couples and families. The role of social workers in working with individuals with SMI also includes conducting psychosocial, cognitive and mental health assessments, and working as part of an interdisciplinary team to develop and support individualized treatment plans. As social workers, our work helps to reduce stigma and promote evidence-based treatment for all persons in need of support. This support may include advocacy work at the mezzo- and macro-levels to address some of the basic human needs of individuals with SMI at the municipal, provincial, and federal levels.
Maternal Mental Health
Having a baby can be an exciting and life affirming experience; however, this is not the experience of all families. The perinatal period is often an overwhelming, stressful and anxiety-inducing time that can affect every aspect of life for the woman, partner and family unit. As a social worker, working in rural and remote locations with families during the perinatal period is recognized as practice that is potentially impacted by great risk, as well as opportunity for the greatest outcomes.
In Canada, one family experiencing PMADs (Perinatal mood and anxiety disorders) is estimated to cost the healthcare system over $150,000. However, by utilizing a simple screening tool and providing access to treatment, the cost is estimated at $5000 (Bauer et al., 2014). As social workers, we also consider the hidden costs that include the impact on the child, mother, family and community. Suicide is the leading cause of death during the perinatal period for women (Bauer et al., 2014; Grigoriadis et al., 2017).
Maternal mental health is defined as “a state of well-being in which a mother realizes her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to her community” (McCauley et al., 2019, p. 2). The term perinatal refers to the period of conception up to and including 12 months after a birth. Perinatal mood and anxiety disorders (PMADs) refer to a variety of mental health issues that fall within the mental health continuum. They include Depression, Bipolar Disorder, Anxiety, Panic Disorder and Obsessive-Compulsive Disorder. In extreme situations, Psychosis can also be included, but this would be classified as a rare medical emergency.
Understanding perinatal mood and anxiety disorders (PMADs) and their origins is as complicated and unique as is the woman and family unit. As a social worker working with new or expecting families, you need to familiarize yourself with the signs and symptoms of PMADs. Risk factors increase or decrease depending on a number of factors that may include social, psychological, environmental, and hormonal issues. Families that are marginalized and experience lower socio-economic status, food insecurity, family violence, adverse life experiences, historical trauma, and are 2SLGBTQ+, are at increased risk of developing PMADs. First Nations women are 20% more likely to have post-partum depression than Caucasian women (Dharma et al., 2019). It’s important to note that not all families who share these particular factors are destined to have PMADs. However, every family is at risk of developing PMADs; for instance, even fathers/partners may experience symptoms of depression after the birth of the baby at a rate of 10% (Paulson & Bazemore, 2010).
The short- and long-term consequences of untreated perinatal mood and anxiety disorders (PMADs) can be detrimental to the woman, baby, family and community. Depression and anxiety can present distinctly for each woman, though some common features include feelings of sadness, lethargy, anger and worry. These are unlike “baby blues” that are shorter in duration and lack physical and emotional intensity. Other outcomes include impact on the partner relationship, attachment issues, as well as social, emotional and cognitive development in the baby (Letourneau et al. 2012).
When reviewing how Canada is doing with respect to maternal mental health (Hippman et al., 2022), research identified numerous gaps and regional differences, and advocates for a national perinatal mental health strategy that would target prevention and triaging into treatment and support. From a social work perspective, this advocacy work is best coordinated at all three service levels (micro, mezzo, and macro).
Parents residing in rural and remote locations are often burdened with travel costs and face the reality of having to leave their other children behind to be tended to by members of the community when they have to access labor and delivery services in larger urban centres. Some rural and remote locations may have a health centre, but due to physician shortages and the lack of locum doctors, families may be directed to another community to access care. Parents experiencing high risk pregnancies are usually directed to leave their home community at 38 weeks gestation or earlier, which can create financial barriers requiring travel and a hotel stay; the parent would then also be in an unfamiliar community without any informal supports (family and friends) to rely upon.
Building maternal mental health capacity in rural and remote locations requires a multi-faceted approach that considers the local culture, community strengths, and opportunities for development. Many remote communities have a long history of childbirth and mental wellness, and each geographic area will have its own ceremonies, traditions and protocols that honour the significance of taking care of the family in a holistic manner. The use and training of doulas and midwives who are connected to the community would be an example of building capacity at the community level, as would training of maternal mental health providers (including social workers) in a manner that is respectful of the traditions and culture of the region. Key social work competencies when working with families during the perinatal period include:
- Treating the family with respect, and honouring their specific cultural needs and requests;
- Providing education on positive mental health and appropriate screening tools;
- Sharing knowledge of both formal and informal supports available in the community to support the family unit; and
- Enhancing the attachment between baby and caregivers.
Violence
Social workers engage with vulnerable populations that are experiencing various challenges, and this includes working with survivors and perpetrators of violence. Regardless of the geographic setting, violence is a multifaceted issue and it has detrimental effects on the individual, family and community. In providing mental health supports, prevention initiatives and intervention services must consider individual, community, and societal factors and how they affect individuals and families experiencing violence. Social workers work collaboratively to initiate life-changing interventions and support mental health on a daily basis, and in rural and remote communities there is always the potential for social workers to find themselves alone in a dangerous situation during such interventions.
The World Health Organization Violence Prevention Alliance divides violence into three sub-types according to the victim-perpetrator relationship: self-directed violence (suicide, suicide attempts and self-abuse), interpersonal violence (youth violence, intimate partner violence, sexual violence, gender-based violence, child maltreatment, and elder abuse), and collective violence (violence committed by larger groups of individuals and can be subdivided into social, political and economic violence) (WHO, 2010). The World Health Organization (2010) also states that violence represents a “major health, criminal justice, human rights, and development challenge” (p. 2). It over-burdens health and mental health systems, undermines communities, and slows economic and social development (WHO, 2010).
Regardless of the type of violence that is impacting communities and mental health, social workers need to be familiar with risk assessment, risk management and safety planning. Conducting a thorough risk assessment of every client is critical, and should always include efforts to determine a prior history of violence, mental illness or other mental health-related challenges, drug and alcohol use, and weapon use. There is no doubt that information and knowledge is powerful when trying to prevent violence, and to mitigate the effects of violence.
When working in remote and rural areas, it is important to build relationships and understand the uniqueness of the community. This includes building knowledge of available resources and programs to support good mental health, and understanding cultural norms that can serve as risk factors or protective factors. Rural and remote communities do not have access to the same formal mental health supports and services as do urban centres.
Geographic isolation can contribute to barriers for those seeking services, such as a lack of transportation and limited access to appropriate resources. Other challenges for individuals who have experienced mental illness, addictions, and violence living in rural and remote areas include greater distances between homes, being less visible to neighbors or other potential witnesses, and being further away from emergency services. In many rural and remote areas there are an abundance of weapons, as well as situations where the justice system allows the return of weapons for hunting season to those charged and convicted with violent offences. Access to e-mail and the Internet, as well as adequate and consistent cell phone coverage, is not available in many areas outside of large urban centres (Kasdorff & Erb, 2010).
Rural communities have unique resources and capacities for mental health resilience such as a tightly knit network of support and a strong relationship to the natural environment (Hirsch & Cukrowicz, 2014). These can be protective factors when one fits in, and they can create a sense of belonging within close, tight-knit communities. However, these same unique resources and capacities can also contribute to a heightened risk of conflict and violence.
As a social worker delivering mental health services in areas outside of large urban centres, you will need to take proactive steps to mitigate violent encounters. First, all practicing social workers must have adequate and responsible supervision and support from a supervisor. This supervision should support ethical considerations and best practice, while instilling a culture of safety and risk reduction. Secondly, social workers should have access to relevant safety training and technology, including GPS tracking. In recent years, there have emerged a number of innovations in mental health service delivery that have the potential to be particularly helpful in rural, remote, and northern environments by creating safe options for clients and social workers outside of large urban settings.
Innovations in Mental Health Service Delivery
Telehealth is an innovation that originally emerged to help bridge the distance for residents living in rural and remote areas in order to access health care. Telehealth is defined as the use of digital information and communication technologies, such as computers and mobile devices, to access personal health care services remotely (Mayo Clinic, 2022). More specific to mental health interventions, telepsychiatry facilitates staff education and specialty consultation; reduces rural practitioners’ sense of isolation; better protects patient anonymity, potentially reduces stigma; generates reliable diagnoses; and yields high patient and provider satisfaction (Hubley et al., 2016).
In addition to more traditional telepsychiatry services, there are other options that have emerged in response to limited accessibility and resources such as telephone helplines, telephone counselling, video counselling, Internet Cognitive Behavioral Therapy (ICBT), walk-in (rapid access) counselling services, mobile apps, and other digital health platforms. The next sections will focus on mobile apps and digital health platforms, as well as walk-in counselling (rapid access) service options.
Mobile Apps and Digital Mental Health Platforms
Mental wellness/health apps and digital mental health platforms have continued to increase in popularity, and are seeing further development and growth as users download them with the hopes of managing and addressing mental health challenges and mental illness such as anxiety and depression (Marshall et al., 2020). Increasingly, governments and service providers are endorsing these options as viable alternatives to face-to-face support due to low cost, convenience, and accessibility (Parker et al., 2019). A number of treatment approaches including cognitive behaviour therapy (CBT), dialectical behaviour therapy (DBT), and prolonged exposure therapy are being assimilated into apps that can stand alone or supplement the face-to-face therapy process (East & Havard 2015).
Mental health apps and digital platforms have the potential to reach people who would otherwise not receive help by removing the barriers to access. These apps and digital platforms may reduce cost, eliminate wait-times, and may also reduce the stigma that can exist for those receiving support for mental health challenges. These support options can promote user autonomy by facilitating self-awareness and self-efficacy, which fits within the realm of social work values. For those outside of large urban centres, mental health apps may also be applied for real-time monitoring of users who are in crisis without available in-person supports (Robillard et al., 2019). Barriers to accessibility of mental health apps and digital platforms, however, exist due to connectivity issues in rural and remote locations, computer and technological literacy issues, as well as costs associated with the purchase of cell phones and computers. There is also a cost associated with accessing the apps themselves.
A lack of privacy can also pose challenges for some who do not have a private place to talk due to others in the home and/or concerns around safety. For some individuals, seeking help can risk their safety and wellbeing. As a result, there are some mental health websites and apps that have a quick exit feature to increase safety for people at risk of, or are experiencing, violence.
Finally, because there are no regulations nor standards in place for mental health apps and digital platforms, they may provide inaccurate information and resources and services that are not evidence-based; which poses ethical concerns from a social work perspective. However, these options continue to be developed and made widely available. The research and literature regarding efficacy of these approaches to support mental health and wellness is limited, but data suggests that this technology is being well-utilized by subscribed users (Marshall et al., 2020; Robillard et al., 2019).
Walk in Counselling (Rapid Access)
Walk in counselling clinics have been operating throughout Canada for over 25 years, and this approach to service delivery is more established in Canada than anywhere else in the world (Hoyt & Talmon, 2014). The rapid access model of counselling is typically implemented to help reduce barriers for individuals seeking support and as a response to diminishing resources (Harper-Jaques & Foucault, 2014). Within rural and remote communities, few affordable counselling services are often available, which can result in people not receiving help when they are seeking it. Again, this may be due to factors such as lack of transportation, length of travel time, lack of child care and/or the stigma related to seeking help. Walk in counselling services have emerged as a creative means to reduce barriers and offer individuals and families help when they need it.
Conclusion
Accessibility is one of the five pillars of the Canada Health Act (Health Canada, 2015), yet many Canadians continue to experience barriers to accessing the care that they need. This is especially true for individuals living in rural, remote, and northern areas in Canada who are seeking mental health supports and treatment options for mental illness. As service providers living and practicing in these communities outside of large urban centres, social workers are well-positioned to provide information, assessments, interventions and ongoing supports to individuals struggling with mental illness and addictions.
This chapter discussed mental health and mental illness, with a particular emphasis on the mental health continuum [MHC] model as a tool to be utilized by social workers in rural and remote settings. An exploration of enablers and barriers to accessing mental health supports was provided, and select mental health issues and challenges that social workers address in rural and remote settings was examined. In particular, suicide prevention and intervention, substance use and addictions, chronic mental illness, maternal mental health, and violence were discussed.
There continues to be stigma associated with mental illness and for those experiencing issues with their mental health. The Mental Health Commission of Canada reports that one in every five Canadians experiences a challenge to their mental health within a given year (MHCC, 2022a). While we often have a good understanding of physical illness, there tends to be less knowledge available about mental illness or substance use issues. As discussed in this chapter, a lack of understanding leads to fear and negative attitudes towards individuals living with mental illness and addictions, and it prevents people from seeking help for themselves and from providing appropriate support to people around them. These issues are even more apparent in rural and remote communities.
Just as social workers provide information, supports, and care to those in rural and remote communities who struggle with challenges to their mental health; social workers who practice in rural and remote settings must also work to maintain their own mental health and wellness. Having the support of colleagues and supervisors can be essential to avoiding burnout for any social worker. However, social workers practicing outside of large urban centres often do not find those connections easy to build. As a result, they must create supportive networks with allied professionals and social workers in different regions in order to access the feedback and collaboration that is needed for their own mental health and wellness. Maintaining good mental health is essential for good social work practice.
Activities and Assignments
- Think about the various stereotypes that you have heard about people experiencing mental illness over your lifetime. Have those stereotypes changed over the years? Which of those stereotypes do you believe are still prevalent for you, or for your family, or in your community? How might these stereotypes affect you as a social worker supporting individuals and families living with mental illness in rural or remote communities?
- What are some of the barriers that individuals seeking help in order to address suicidal thoughts in rural and remote locations might encounter? What are some of the enablers that might support a suicidal individual in seeking mental health support?
- Online peer support can be beneficial for the person with serious mental illness (SMI) living outside of an urban centre. As the social worker supporting this individual utilizing online peer support, what factors would you need to consider to mitigate potential risk to the individual?
- Identify a rural or northern community that you are familiar with, and list the services that are available there to support maternal mental health. What barriers to good mental health for a family with a newborn might be present in that same community?
Additional Resources
- Mental Health Commission of Canada [MHCC]. (2021). Answering the call: Strategic plan 2021/2030. Available on the Mental Health Commission of Canada website.
References
Allport, G.W. (1937). Personality: A psychological interpretation. Holt.
American Psychiatric Association [APA]. (2021). Diagnostic and statistical manual of mental disorders (DSM-5), fifth edition. Author.
American Society of Addiction Medicine. (2019). Definition of addiction. https://www.asam.org/quality-care/definition-of-addiction
Baxter, L., Burton, A., & Fancourt, D. (2022). Community and cultural engagement for people with lived experience of mental health conditions: What are the barriers and enablers? BMC Psychology, 10(71).
Bauer, A., Parsonage, M., Knapp, M., Iemmi, V., & Adelaja, B. (2014). The costs of perinatal mental health problems. Centre for Mental Health and London School of Economics.
Brands, B., Di Ciano, P., & Mann, R.E. (2021). Cannabis, impaired driving and road safety: An overview of key questions and issues. Frontiers in Psychiatry, 12, 641549.
Canadian Association of Social Workers [CASW]. (n.d.). The role of social work in mental health.
Canadian Centre on Substance Use and Addiction [CCSA]. (2019). Canadian drug summary: Summer 2019. Author. ISBN 978-1-77178-583-9
Canadian Mental Health Association [CMHA]. (2021). Mental health and mental illness: What’s the difference? https://cmha.ca/brochure/fast-facts-about-mental-illness/
Canadian Mental Health Association [CMHA] Ontario. (2009). Backgrounder: Rural and northern community issues in mental health. https://ontario.cmha.ca/wp-content/uploads/2009/09/cmha_on_rural_northern_mental_health_issues_20090827.pdf
Canadian Mental Health Association [CMHA] Ontario. (2022). Stigma and discrimination. https://ontario.cmha.ca/documents/stigma-and-discrimination/
Chen, S.P., Chang, W.P., & Stuart, H. (2020). Self-reflection and screening mental health on Canadian campuses: Validation of the mental health continuum model. BMC Psychology, 8(76).
Chowdhury, M.R. (2021). What is the mental health continuum model? https://positivepsychology.com/mental-health-continuum-model/
Cleary, A. (2012). Suicidal action, emotional expression, and the performance of masculinities. Social Science & Medicine, 74(4), 498-505.
Creighton, G., Oliffe, J., Ogrodniczuk, J., & Frank, B. (2017). "You've gotta be that tough crust exterior man": Depression and suicide in rural-based men. Qualitative Health Research, 27(12), 1882-1891.
Dharma, C., Lefebvre, D.L., Lu, Z., Lou, W., Becker, A.B., Mandhane, P.J., Turvey, S.E., Moraes, T.J., Azad, M.B., Chen, E., Elliott, S.J., Kozyrskyj, A.L., Sears, M.R., & Subbarao, P. (2019). Risk for maternal depressive symptoms and perceived stress by ethnicities in Canada: From pregnancy through the preschool years. Canadian Journal of Psychiatry, 64(3), 190–198.
Dudley, J.R. (2000). Confronting stigma within the services system. Social Work, 45, 449-455.
Dykxhoorn, J., Hollander, A.C., Lewis, G., Dalman, C., & Kirkbride, J.B. (2019). Family networks during migration and risk of non-affective psychosis: A population-based cohort study. Schizophr Res, 208, 268-275.
East, M., & Havard, B. (2015). Mental health mobile apps: From infusion to diffusion in the mental health social system. JMIR Mental Health, 2(1).
Franken, K., Lamers, S.M.A., Ten Klooster, P.M., Bohlmeijer, E.T., & Westerhof, G.J. (2018). Validation of the Mental Health Continuum-Short Form and the dual continua model of well-being and psychopathology in an adult mental health setting. Journal of Clinical Psychology, 74, 2187–2202.
Frederick, L. (2020). Barriers to help-seeking in men for mental health issues: The impact of gender role socialization and masculine ideologies. [Master’s thesis, The City University of Seattle]. Digital Archive.
Friesen, E. (2019). The landscape of mental health services in rural Canada. UTMJ, 96(2), 47-52.
Goffman E. (1963). Stigma: Notes on the management of spoiled identity. Simon & Schuster.
Greene, K.M., Murphy, S.T., & Rossheim, M.E. (2018). Context and culture: Reasons young adults drink and drive in rural America. Accident Analysis and Prevention, 121, 194-201.
Grigoriadis, S., Wilton, A.S., Kurdyak, P.A., Rhodes, A.E., Vonder Porten E.H., Levitt, A., Cheung, A., & Vigod, S.N. (2017). Perinatal suicide in Ontario, Canada: A 15-year population-based study. CMAJ, 189(34), E1085-E1092.
Harper-Jaques, S., & Foucault, D. (2014). Walk-in single-session therapy: Client satisfaction and clinical outcomes. Journal of Systemic Therapies, 33, 29-49.
Health Canada. (2015). Canada Health Act: Annual Report (2014-2015). HC Pub: 150140.
Herek, G.M. (2002). Thinking about AIDS and stigma: A psychologist’s perspective. The Journal of Law, Medicine & Ethics, 30, 594–607.
Hippman, C.L., Adham, M., Zlobin, C., & Wong, G. (2022). An environmental scan of perinatal mental health infrastructure across Canada. Journal of obstetrics and gynaecology Canada, 44(7), 745-746.
Hirsch, J., & Cukrowicz, K. (2014). Suicide in rural areas: An updated review of the literature. Rural Mental Health, 38(2).
Hoyt, M.F., & Talmon, M. (Eds.). (2014). Capturing the moment: Single session therapy and walk-in services. Crown House Publishing Limited.
Hubley, S., Lynch. S.B., Schneck, C., Thomas, M., & Shore J. (2016). Review of key telepsychiatry outcomes. World J Psychiatry, 6(2), 269-82.
Irvine, J., & Quinn, B., (2017). Northern Saskatchewan health indicators, health status: Mortality. Athabasca Health Authority, Keewatin Yatthé Health Region and Mamawetan Churchill River Health Region. Population Health Unit, La Ronge, SK.
Jones, M.K., & Quinn, M.A. (2021). Buprenorphine–naloxone induction in the north. Can J Rural Med, 26, 35-7.
Kasdorff, D., & Erb, B. (2010). Serving victims of violence in rural communities: Challenges and best practices. Victim/Witness Assistance Program, East Region, Ontario.
Kirby, M.J., & Keon, W.J. (2006). Out of the shadows at last: Transforming mental health, mental illness and addiction services in Canada. Report of the Standing Senate Committee on Social Affairs, Science and Technology, Government of Canada.
Kitchen, P., Williams, A., & Chowhan, J. (2012). Sense of community belonging and health in Canada: A regional analysis. Social Indicators Research, 107, 103-126.
Letourneau, N.L., Dennis, C.L., Benzies, K., Duffett-Leger, L., Stewart, M., Tryphonopoulos, P.D., Este, D., & Watson, W. (2012). Postpartum depression is a family affair: Addressing the impact on mothers, fathers, and children. Issues in Mental Health Nursing, 33(7), 445-457.
Lister, K., Seale, J., & Douce, C. (2021). Mental health in distance learning: A taxonomy of barriers and enablers to student mental wellbeing. The Journal of Open, Distance and e- Learning,
MacLeod, M.L.P., Penz, K.L., Banner, D., Jahner, S., Koren, I., Thomlinson, A., Moffitt, P., & Labreque, M.L. (2022). Mental health nursing practice in rural and remote Canada: Insights from a national survey. International Journal of Mental Health Nursing, 31, 128-141.
Marshall, J.M., Dunstan, D.A., & Bartik, W. (2020). Effectiveness of using mental health mobile apps as digital antidepressants for reducing anxiety and depression: Protocol for a multiple baseline across-individuals design. JMIR Research Protocols, 9(7), e17159.
Mate, G. (2011). Close encounters with addiction. Central Recovery Press.
Mayo Clinic. (2022). Telehealth: Technology meets healthcare. Health Information. https://www.mayoclinic.org/healthy-lifestyle/consumer-health/in-depth/telehealth/art-20044878
McCauley, M., Brown, A., Ofosu, B., & van den Broek, N. (2019). “I just wish it becomes part of routine care”: Healthcare providers’ knowledge, attitudes and perceptions of screening for maternal mental health during and after pregnancy: A qualitative study. BMC Psychiatry, 19(279), 1-8.
Mental Health Commission of Canada [MHCC]. (2022a). Mental Health First Aid: Program history. https://mentalhealthcommission.ca/training/mhfa/program-history/
Mental Health Commission of Canada [MHCC]. (2022b). How alcohol and suicide are connected - a fact sheet. https://mentalhealthcommission.ca/resource/alcohol-use-and-suicide-fact-sheet/
Naslund, J., Grande, S., Aschbrenner, K., & Elwyn, G. (2014). Naturally occurring peer support through social media: The experiences of individuals with Severe Mental Illness using YouTube. PLoS ONE, 9(10), e110171.
National Alliance to End Rural and Remote Homelessness [NAERRH]. (2021). Rural & remote homelessness: A call for strategic investments in rural and remote communities across Canada.
National Institute on Drug Abuse [NIDA] (2021). Opioid overdose crisis. https://nida.nih.gov/drug-topics/opioids/opioid-overdose-crisis
NSCAD (2021). Peer mentors: Self monitoring with the mental health continuum tool. NS: NSCAD University. https://navigator.nscad.ca/wordpress/wp-content/uploads/2021/10/Mental-Health-Continuum-Tool-PDF-EDIT.pdf
Park, J., Tjepkema, M., Goedhuis, N., & Pennock, J. (2015). Avoidable mortality among First Nations adults in Canada: A cohort analysis. Health Reports, 26(8), 10-6.
Parker, L., Halter, V., Karliychuk, T., & Grundy, Q. (2019). How private is your mental health app data? An empirical study of mental health app privacy policies and practices. International Journal of Law and Psychiatry, 64, 198-204.
Paulson, J., & Bazemore, S. (2010). Prenatal and postnatal depression in fathers’ and its association with mental depression: A meta-analysis. Journal of the American Medical Association, 303(19), 1961-1969.
Perreault, S. (2019). Police-reported crime in rural and urban areas in the Canadian provinces, 2017. Juristat, Canadian Centre for Justice Statistics, 1, 3-37.
Persson, L. Dobson, K.S., & Frampton, N.M.A. (2021). Evaluation of a mental health continuum model in two samples. Canadian Journal of Behavioural Science, 54(3), 206–212.
Pijl, E.M., Alraja, A., Duff, E., Cooke, C., Dash, S., Nayak, N., Lamoureaux, J., Poulin, G., Knight, E., & Fry, B. (2022). Barriers and facilitators to opioid agonist therapy in rural and remote communities in Canada: An integrative review. Substance Abuse Treatment, Prevention, and Policy 17, 62 (2022).
Reccord, C., Power, N., Hatfield, K., Karaivanov, Y., Mulay, S., Wilson, M., & Pollock, N. (2021). Rural–urban differences in suicide mortality: An observational study in Newfoundland and Labrador, Canada. The Canadian Journal of Psychiatry, 1-11.
Robillard, J.M., Feng, T.L., Sporn, A.B., Lai, J., Lo, C., Ta, M., & Nadler, R. (2019). Availability, readability, and content of privacy policies and terms of agreements of mental health apps. Internet Interventions: The Application of Information Technology in Mental and Behavioural Health, 17, 1-8.
Schmidt, G. (2008). Professional work in remote, northern communities: A social work perspective. UNBC Community Development Institute.
Slaunwhite, A.K., & MacDonald, S. (2015). Alcohol, isolation, and access to treatment: Family physician experiences of alcohol consumption and access to health care in rural British Columbia. The Journal of Rural Health, 31(4), 335-345.
Smith, T., McNeil, K., Mitchell, R., Boyle, B., & Ries, N. (2019). A study of macro-, mezzo- and micro- barriers and enablers affecting extended scopes of practice: The case of rural nurse practitioners in Australia. BMC Nursing, 18(14), 1-12.
Statistics Canada. (2019). Health fact sheets: Heavy drinking, 2018. Author.
Steele, L.S., Durbin, A., Lin, E., Victor, J.C., Klein-Geltink, J., & Glazier, R.H. (2014). Primary care reform and service use by people with serious mental illness in Ontario. Healthcare Policy, 10(1), 31- 45.
Vakharia, S.P., & Little, J. (2017). Starting where the client is: Harm reduction guidelines for clinical social work practice. Clinical Social Work Journal, 45, 65–76.
Wang, Y., Feng, Y., Han, M., Duan, Z., Wilson, A., Fish, J., Sun, S., & Chen, R. (2021). Methods of attempted suicide and risk factors in LGBTQ+ youth. Child Abuse & Neglect, 122.
Westhues, A., Lafrance, J., & Schmidt, G. (2001). A SWOT analysis of social work education in Canada, Social Work Education, 20(1), 35-56.
World Health Organization [WHO]. (2021). WHO urges more investments, services for mental health.
World Health Organization [WHO]. (2017). Depression and other common mental disorders: Global health estimates.
World Health Organization [WHO]. (2010). Violence Prevention Alliance: Conceptual framework – November 2010. Geneva, Switzerland.
World Health Organization [WHO] (2001). World Health Report 2001. Mental health: New understanding, new hope. Geneva, Switzerland.
This chapter provides an overview of social work practice focused on the delivery of mental health services in rural, remote, and northern communities. As social workers, we know that the prevalence, scope, and range of mental health issues in locations outside of urban centres is significant, and has an impact on the lives of individuals, families and communities. We also know that populations living in these communities don’t always have adequate and necessary access to mental health services and supports. In efforts to fill existing gaps in mental health services, social workers living and practicing outside of urban centres are required to work collaboratively and creatively, while utilizing generalist social work practice skills. Increasingly, mental health issues are a growing public health concern in Canada, with mental illness now identified as one of the leading causes of disability (Chen et al., 2020).
This chapter will highlight the characteristics of rural, remote and northern communities that affect mental health service delivery from a social work perspective; it also discusses select mental health-related issues. Attitudes and beliefs that result in stigma related to mental illness, and towards those experiencing mental health challenges, will also be explored.
Learning Objectives
By the end of this chapter you will have had the opportunity to:
- Understand the scope of practice of social workers providing mental health support services in rural, remote and northern settings.
- Describe factors influencing mental health and addictions outside of urban settings.
- Identify common types of mental health concerns found in rural, remote, and northern settings.
- Understand the barriers and enablers for social workers at the micro-, mezzo- and macro-levels of mental health service provision in rural, remote, and northern settings.
- Recognize how the stigma surrounding mental illness affects service access in locations outside of urban settings, and how to identify strategies to reduce that stigma.
What is Mental Health?
The World Health Organization (2021) stresses the importance of understanding mental health as not just the absence of mental illness, but as a concept that applies to everyone under a range of circumstances. The World Health Organization [WHO] defines mental health as a state of well-being in which the individual realizes their own abilities, can cope with regular stresses of life, can work productively, and is able to make a contribution to their community (2021). The Canadian Mental Health Association [CMHA] describes mental illness as a disturbance in thoughts, feelings, and perceptions that is severe enough to affect everyday functioning. Some examples of mental illnesses are anxiety disorders, schizophrenia, and mood disorders such as major depressive disorder and bipolar disorder. Substance misuse is often linked to poor mental health or mental illness (CMHA, 2021). Internationally, and in most jurisdictions across Canada, supports and services are often offered to address both mental health- and addictions-related issues. In the literature, and in practice, mental illness is sometimes referred to as: mental conditions, mental health issues, mental health difficulties, psychological disorders, and challenges to mental health (Baxter et al., 2022; Chen et al., 2020; Lister et al., 2021).
The Mental Health Continuum Model
Within mental health service delivery, the mental health continuum [MHC] model refers to a specific model that has been developed to help with understanding mental health that incorporates a self-help tool. This model is used to:
- Identify the underlying causes of impairment in daily-life functioning;
- Gather information about mental health of individuals over time;
- Indicate when it would be ideal to seek professional assistance for restoring balance in mental health; and
- Learn how to recognize symptoms of psychological disorders (Chowdhury, 2021).
Originally developed by the Canadian Armed Forces [CAF], the MHC model describes four main states of mental health a person could possibly experience. The model is presented as a continuum, which means that a person can move back and forth along the continuum scale and can also land somewhere between the four main areas at any given time (Chen et al., 2020; NSCAD, 2021).
Figure 1
In a more general sense, the mental health continuum refers to a range of mental wellbeing with mental health and mental illness at the two extreme ends. Depending upon the circumstances of an individual at any given point in time, he/she/they can be situated at one point of the continuum but can actually shift position as their situation improves or deteriorates, which is seen as being an effective way to interpret mental health (Allport, 1937; Chen et al., 2020). Consistent throughout the literature is the acknowledgement that there is a place for everyone on the mental health continuum (Chen et al., 2020; Chowdhury, 2021), and that this approach can potentially reduce stigma due to the idea that everyone fits in. The model is intended to serve as a self-reflection and self-monitoring tool, with colours indicating the level of severity of illness. By incorporating colours, the intention is to further reduce stigma by limiting use of jargon and reducing the potential impact of diagnostic labels (Chen et al., 2020). The MHC model has been adopted widely as a tool to promote mental health in various settings and contexts in Canada and internationally (Chen et al., 2020; Franken et al., 2018). The mental health continuum short form [MHC-SF] has been validated in nonclinical samples and incorporated in various countries and cultures (Franken et al., 2018).
Social Workers and the Mental Health Continuum Model
An approach to practice that incorporates the MHC model can be helpful for social workers, regardless of practice setting. However, especially in rural, remote, and northern communities, this model can help social work practitioners to recognize specific behavioral patterns in clients that may need attention and allow them to suggest ways of dealing with service needs in creative ways. Creative approaches and out-of-the-box thinking can be helpful in settings that lack a comprehensive range of formal mental health supports.
For practicing social workers, this model can also offer helpful information to consider as they strive to maintain their own mental health and wellness by serving as a practical and reliable tool for social workers to identify their own sources of personal and professional stress by:
- Understanding how to identify symptoms of mental illness in oneself and others;
- Encouraging the growth and maintenance of a healthy mindset that can assist in overcoming distress and create positive movement on the continuum; and
- Learning how to deal with psychological and emotional crises effectively while not allowing one’s well-being to be jeopardized (Chowdhury, 2021).
Generalist Social Work Practice in Mental Health Service Delivery
Undergraduate social work programs across Canada and North America focus on a generalist approach to social work practice (Weshues et al., 2001). This approach equips social workers with information on the basic concepts in social work, as well as a range of skills and a level of awareness that prepares them for a variety of social work roles in a range of settings. By focusing on generalist practice, students are introduced to ideas that include the promotion of well-being and the application of preventative and intervention methods to address social problems at individual (micro), group (mezzo), and community (macro) levels (Weshues et al., 2001). Although these levels are often spoken of as distinct, they actually occur in tandem and are linked to, and constantly influence, one another.
Rural, remote and northern locations offer unique opportunities for practicing social workers. In fact, many new social workers seek employment in these settings in order to gain practical experience in a relatively short period of time (Schmidt, 2008). Social workers in urban settings will tend to work in areas of practice considered to be more focused and specialized, whereas settings outside of urban areas require the social worker to engage in a number of areas of practice simultaneously. These areas of practice may include child protection services, addictions, mental health, income support, community development, and policy.
Mental Health Enablers and Barriers outside of Urban Settings
As discussed previously in this book, individuals who live outside of urban centres face unique factors that impact directly upon everyday life. While the quality of life in rural, remote and northern communities is idyllic in many ways, and is often sought after, the challenges associated with living outside of large centres can also affect that quality of life in negative ways – especially in relation to mental health. These negative effects include:
- Less comprehensive, available, and accessible support services,
- Transportation limitations due to geographic accessibility,
- Fragmented continuity of care,
- Difficulties with workforce recruitment and retention,
- Lack of access to affordable housing, and
- Limited access to population-based funding (CMHA Ontario, 2009).
In this context, a barrier to access is understood as any process or intervention by which access to mental health supports is impeded. Enablers are defined as any process or intervention by which access to mental health services and wellbeing is facilitated (Baxter et al., 2022; Lister et al., 2021). Figure 2 provides an overview of enablers and barriers to accessing mental health supports in rural, remote, and northern communities.
Figure 2
Enablers and Barriers to Mental Health Support Availability outside of Urban Settings
Rural, remote, and northern communities are not homogenous. The populations of people who live in these communities are diverse and represent distinct cultures, ethnicities, ages, and backgrounds. Despite this diversity, most individuals seeking supports and services for mental illness experience widespread stigma regardless of their backgrounds (Friesen, 2019; MacLeod et al., 2022).
Mental Health Issues and Stigma
The concept of stigma has been well-researched over the past 6 decades and has led to the conceptualization of stigma as a social construct. Dudley (2000) defined stigma as “stereotypes or negative views attributed to a person or groups of people when their characteristics or behaviors are viewed as different from, or inferior to, societal norms” (p. 449). These views may focus on what are seen to be mental, physical, or social deficiencies (CMHA Ontario, 2022). Stigma differs from discrimination, which is viewed as unfair treatment due to a person’s identity. This identity can include race, ancestry, place of origin, colour, ethnic origin, citizenship, creed, sex, sexual orientation, gender identity, gender expression, age, marital status, family status or disability, including mental disorder (CMHA Ontario, 2022). In other words, stigma is the negative stereotype, and discrimination is the behaviour that results from this negative stereotype.
It is important to note that, because stigma is a social construct, it changes over time. What was stigmatized in the past may not be stigmatized today, or has changed in terms of how it is expressed at the micro-, mezzo- and macro-levels. This change often will occur as a shifting between the three levels. Goffman (1963) referred to this as the “process of devaluation” (p. 3), which can dehumanize anything or anyone that sits outside the lines of what the community believes to be acceptable. This process can create an “us versus them” scenario that is founded in difference, stereotypes, and misinformation; it can result in fear leading to unfair treatment of individuals. In a rural or remote community, this discrimination can be devastating, as an already small social network can become yet smaller, or even non-existent.
Stigma related to mental illness and mental health issues can have detrimental consequences. The World Health Organization [WHO] (2001) has suggested that stigma is one of the largest barriers to mental illness treatment engagement, despite the fact that treatment has been shown to be effective. Due to stigmatization, people may delay seeking help, may exit treatment prematurely, or may completely avoid seeking services. These realities will often increase psychological distress and when individuals can no longer wait due to an increase in symptoms, the level of distress is significantly greater. Stigma can impact social activities for individuals experiencing mental illness, along with education, housing, and employment; the result is often social isolation. Herek (2002) stated: “stigma and discrimination are the enemies of public health” (p. 604). Stigma in the rural and remote areas of Canada can be further compromised by a shortage of services in the areas of mental health and addictions, and difficulty in accessing those services. Stigma at the micro-, mezzo- and macro-levels, in conjunction with a lack of formal supports, can leave people in a very precarious position.
Social workers work with a variety of complex cases that require a thoughtful approach. Working in rural and remote areas with under-served populations requires the social worker to have a sophisticated level of knowledge and understanding of mental health and mental illness, as well as ethical fortitude. Further, a knowledge base of the current and historical culture of the geographic region in which they are practicing is critically important. No two communities are the same and each will have distinct enablers and protective factors, as well as specific barriers and factors that may put people at greater risk. An insular community may have a variety of protective and enabling factors, but someone who is marginalized within that community may also feel like an outsider. This experience will undoubtedly affect that individual’s mental health. Social workers working in rural and remote communities have a unique opportunity to influence efforts to de-stigmatize mental illness. They will work with individuals and their families and can mitigate stigma at the micro- and mezzo-levels. For example, involving the family will support the individual with mental illness, and help the family to understand conditions impacting mental health; this can re-build the family structure and support system. On a macro-level, the social worker will have opportunities to support educational efforts to de-stigmatize mental illness and advocate for local and regional changes. They can advocate for policy change, and ensure that mental health policy is being developed at the same time and rate as health policy. Through the nature of their generalist practice approaches, social workers will also be networking with various agencies and can be an agent of change to support community-wide mental health and wellness initiatives.
A social worker working in mental health services requires the ability to self-reflect about their own stereotypes, beliefs and prejudices. It is also important to acknowledge that we, the community in which we serve, as well as the person in need; all have known and unknown attitudes about what they are coming to discuss. We must create a space where these attitudes and beliefs can be explored and tested, in order to determine their impact on services.
Areas of Practice in Mental Health Services
As discussed throughout this book, a social worker engaging in practice outside of urban settings will have many opportunities to work with a range of individuals from diverse backgrounds. These individuals will seek support services from social workers in order to deal with many aspects of mental health and mental illness. This section will focus on five select areas of social work practice specific to mental health in rural and remote settings: suicide prevention and intervention, substance use and addictions, chronic mental illness, maternal mental health, and violence.
Suicide Prevention and Intervention
In Canada, suicide is identified as the ninth leading cause of death among the general population. However, for individuals between the ages of 15 and 34, suicide is the second leading cause of death (MHCC, 2022b). In first world countries, men are three times more likely than women to die by suicide (WHO, 2017). Lesbian, gay, bisexual, transgender, queer/questioning and other sexual and gender minority (2SLGBTQ+) youth have also been consistently identified as having an elevated risk for suicide (Wang et al., 2021).
The Mental Health Commission of Canada (2022b) reports that alcohol abuse is the second most common mental health problem identified in people who die by suicide, and one in four deaths by suicide are completed by those who abused alcohol. Suicide rates are also higher in rural areas as compared to urban areas (Creighton et al., 2017; Frederick, 2020; Reccord et al., 2021). The rates of suicide in Canada are consistent with suicide rates in other first world countries that experience similarities in terms of poverty levels, aging populations, lack of employment opportunities, and out-migration to urban centres (Cleary, 2012).
Suicide has had a profound impact on communities that are predominantly First Nations, Métis and Inuit. In fact, the suicide rates among First Nations and Métis adults have been reported to be twice as high as among non-Indigenous adults (Park et al., 2015). The rates of suicide in Northern Saskatchewan are very high, and suicide is identified as the leading cause of death for people aged between 10 years to 40 years (Irvine & Quinn, 2017). Suicide intervention approaches need to be culturally responsive in areas that have a higher First Nation, Métis and Inuit population; where the impacts of colonization and inter-generational trauma are the predominant underlying factors impacting suicide rates.
Suicide prevention strategies should be targeted to the local demographics and culture in rural and remote communities, and designed by local stakeholders with a focus on community needs and assets. Social workers can play an important role in suicide prevention, education, and intervention.
Suicide in in rural and remote areas is of significant concern, yet populations impacted by suicide continue to be overlooked and underserved at all three levels of intervention (micro, mezzo, and macro). A review of the literature by Hirsch and Cukrowicz (2014) identified that successful interventions require a thoughtful approach which focuses on the geographic location, social belief systems, and determinants of health that impact suicide. It is also important to recognize the effects of poverty and lack of employment opportunities, as well as the importance of creating literacy around mental wellness and building trauma-informed communities.
As social workers, we have to pay attention to social, cultural, and economic-specific strengths and adversities of communities, as well as social and cultural norms. Every rural or remote community will have its own nuances about what is stigmatizing, its own history within Canada, and its own trauma legacy.
Substance Use and Addictions
Addictions can affect anyone. The Canadian Mental Health Association estimates that approximately 21% of the Canadian population (about 6 million people) will meet the criteria for addiction at some point in their lifetime (CMHA, 2022). Alcohol is identified as the most common drug used by Canadians, and those living in rural and remote areas of the country were more likely to report heavy drinking compared to those living in urban areas (CCSA, 2019; Statistics Canada, 2019).
The American Society of Addiction Medicine (2019) defines addiction as “a treatable, chronic medical disease involving complex interactions among brain circuits, genetics, the environment, and an individual’s life experiences”. The topic of addictions is vast as it includes the abuse of illegal substances, the misuse of legal substances, as well as compulsive behaviors involving gambling, internet/gaming, and sex. As social workers, it is important to be aware of language and how that language is used in this area of practice. In the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders [DSM-5] (APA, 2021), revisions were made to include Substance-Related and Addictive Disorders with substantive changes to the disorders grouped there, plus changes to the criteria of certain conditions. The DSM-5 explains that the essential feature of a substance use disorder is that it includes a cluster of cognitive, behavioral, and physiological symptoms highlighting that with this disorder, the individual continues using the substance despite significant substance-related problems (APA, 2021). In other words, people with addictions use substances or engage in behaviors that become compulsive and often continue the behaviors despite harmful consequences.
Understanding the complexity of addiction is essential for social workers and those working to support individuals with addictions; Gabor Mate (2011) explains that addiction is more than a disease or human choice, it is a response to human suffering. Using substances may provide the person temporary relief from emotional and physical pain, however it can exacerbate the problem and have harmful impacts on one’s health, relationships, work/responsibilities, finances, and may lead to legal problems.
The misuse of alcohol and drugs is influenced by individual, cultural and social factors which can serve as protective and/or risk factors (enablers and barriers). These factors need to be considered when working with individuals and families as part of preventative programming, intervention/treatments and rehabilitation processes. For social workers working in rural and remote areas with people and communities experiencing addiction, consideration of these factors is essential to the working relationship and change process. First, the rural and remote location must be acknowledged and considered, as these places throughout Canada do not have the same access and availability of services as do urban centres. This can be challenging for individuals and families experiencing concerns with mental health and substance use as it may require additional time and financial resources in order to connect with supports; all which can further complicate one’s physical, social and mental wellbeing.
Telehealth services and online programming are often options that can be beneficial for individuals and families living in rural and remote communities, as these options create possibilities for people to connect with informal and formal supports in order to address physical health concerns, as well as mental health concerns. An example of services being utilized in this way can be found in remotely delivered Alcoholics Anonymous or Narcotics Anonymous group meetings. Online meetings allow people more options to attend virtual gatherings that support their schedule, can reduce the need to travel long distances, and also can provide greater anonymity. Although this modality of service may increase accessibility for some, it is not always possible for others as this approach requires internet access, computer literacy skills and a safe and quiet space to connect. Understanding how these factors can be barriers is essential to the helping process.
Individuals misusing substances can be at different stages in their use and readiness for change. A harm reduction approach includes strategies to reduce individual harm through managed consumption and overdose prevention sites. This approach, which was initially developed in the 1980s, recognizes the individual and meets them “where they are at” to help reduce harm, address basic needs, and increase safety and wellness. This approach to service delivery also increases engagement of clients, and supports willingness to change. Harm reduction and social work share common values and approaches, not the least of which is recognizing the client (service-user) as expert, and using strengths-based efforts to build collaborative working alliances (Vakharia & Little, 2017).
Navigating the system to help support individuals with substance use disorders can be especially challenging in rural and remote locations, due to limited outpatient and inpatient services and waitlists. It is important for social workers to understand how social and health determinants contribute to risk, to the treatment of substance misuse, as well as overall wellbeing.
As discussed earlier, individuals living in rural and northern locations report high levels of excessive use of alcohol. Higher rates of driving while impaired is also common. In recent years, opioid use has emerged as a crisis across Canada, and this issue is especially difficult to address in rural and northern communities. These two types of addictions will be discussed further below, as will the issue of impaired driving.
Alcohol
Accessibility and availability of resources for alcohol abuse prevention, intervention and recovery are influenced by social and cultural factors. Poor socio-economic conditions found in many rural communities is correlated with higher levels of alcohol consumption, psychosocial stress, and decreased physical activity and preventive service use (Smith et al., 2019). The limited resources available create an additional challenge when trying to arrange services that are appropriate and meet the individual’s needs. Rural physicians show an awareness and concern for alcohol consumption in their communities, but they also report difficulties in accessing resources to refer patients for substance use treatment (Slaunwhite & MacDonald, 2015).
Communities with smaller populations and/or communities that are located in isolated areas can create more familiarity for individuals. This factor can be understood as both an enabler and as a barrier when it comes to seeking support services. Familiarity may bring people a sense of belonging and support, yet it can also be isolating for those who don’t fit the identified community norms and expectations. The lack of anonymity can prevent individuals and families from seeking help due to shame and stigma. Stigma continues to be a factor that potentially isolates people experiencing difficulties with substance use.
It may be helpful for social workers to consider a social-ecological perspective for explaining influences on alcohol use. Individual-level factors that influence alcohol use are found within home, work, and school environments, which are located within the larger community. Macro-level factors, such as exposure to advertising, may influence family and peer network attitudes and norms, which ultimately impact individual attitudes and behaviors. Social work focuses on the person within their environment and recognizes the importance of family, community, culture, legal, social, spiritual, and economic influences that impact well-being of individuals, families, groups, and communities.
Opioids
There is an opioid crisis affecting communities across Canada (Pijl et al., 2022). This crisis is affecting individuals, families, and communities, often resulting in long term health issues like HIV and hepatitis, possible overdose, and death.
Jones and Quinn (2021) illustrate the impact of remote geography on clinical decisions, adequate medication supply, and the importance of engaging pharmacy and nursing colleagues in delivering addictions care specific to the use of opioids. National practice guidelines for opioid use disorder recommend buprenorphine–naloxone as a first‑line treatment. In rural areas, medications that can be administered on a monthly basis, like buprenorphine and/or naltrexone formulations, might be particularly effective since distance and transportation can present barriers to daily-dose treatment approaches (NIDA, 2021). Clinical practice guidelines state that methadone maintenance therapy (MMT) is the standard of care for treating patients with opioid dependence. Methadone maintenance therapy is a substitution/maintenance treatment model whereby methadone is administered in a structured treatment environment to reduce or eliminate the uncontrolled use of illicit opioids (NIDA, 2021).
Impaired Driving
Research has shown that rates of impaired driving tend to be about twice as high in rural areas as compared to urban areas (Perreault, 2019). For the purpose of this discussion, impaired driving refers to driving while under the influence of alcohol, cannabis, or other mind-altering substances. Greene et al. (2018) found that these rates were often higher in younger age groups and identified specific factors that contribute to those higher rates: social context (peer pressure and parental modeling), rural cultural values (independence, stoicism, and social cohesion), as well as the realities of the legal and physical environment (minimal police presence, sparse population, and no alternative transportation). Since 2018 when Canada became the second country to legalize non-medical cannabis, emerging research has confirmed that driving under the influence of cannabis is an increasingly prevalent road safety issue (Brands et al., 2021). As discussed earlier, higher rates of cannabis and alcohol use are also linked to increased suicidal ideation in young people. Suicidal ideation, or suicidal thoughts, means having thoughts or ideas about the possibility of ending one's own life.
Social workers practicing outside of large urban centres play a key role in working with individuals with substance use and co-occurring disorders, as well as their families and communities. As such, knowledge about substances, behavioral indicators of substance use, relevant assessment tools, and knowledge about available and accessible treatment and support options is essential.
Chronic Mental Illness
Long-term and chronic mental illness is multi-faceted and complex, requiring a coordination of support and collaboration at all three levels of social work practice (micro, mezzo and macro) beginning when the individual seeks ongoing support, and continuing as they enter into the recovery and long-term support process. Most often in the literature, those with chronic mental illness are identified as individuals with Serious Mental Illness (SMI) (Steele et al., 2014), and this is the term that will be used in this discussion. Individuals with SMI fall at the extreme right side of the mental health continuum and may require a greater level of tertiary care in order to stabilize their mental illness and avoid further deterioration. Those with SMI usually require long-term medication and support, and this can include schizophrenia and schizophrenic‐like disorders, but can also refer to any reoccurring mental illness that produces serious functional impairment and interferes with the person’s quality of life including psychosis and bipolar disorders (Steele et al., 2014). Individuals with SMI typically experience gaps in services and these gaps are more pronounced in rural and remote locations that lack community resources and in-patient capacity.
Individuals with SMI tend to socially isolate themselves and this can have compounding effects on the course of their recovery. A supportive and resourced community can have significant and positive influence on the lives of people living with SMI. Protective factors increase when the social capital of the community is more robust. Social capital includes friends, social norms, networks of support and employment opportunities for the individual with Serious Mental Illness in the community (Dykxhoorn et al., 2019), and can play an important role in the person’s overall mental health and physical wellbeing. Social capital also includes the infrastructure of a community such as parks, libraries and other pro-social activities like volunteering opportunities. In their research, Kitchen et al. (2012) found a very strong association between health (mental health in particular) and a sense of belonging, especially in rural areas of Canada.
Peer support can have a positive impact on the person with SMI, as well as the family who may struggle with their own perceptions of mental illness. Peer support can include group activities, mentoring, and a system of mutual giving and receiving where individuals with SMI can offer hope, companionship, and encouragement to others facing similar challenges (Naslund et al., 2014). Peer support lays primarily in the mezzo-level of support provided by social workers, and can have a significant impact on the micro-level as the social capital increases and the person’s sense of inclusion and community belonging also increase. Individuals with SMI often turn to social media to seek information and create communities to share their experience, and to obtain information from others with a similar diagnosis. This network building can significantly reduce personal and social stigma and normalize experiences as they increase insight about their diagnosis, develop on online community where potentially none exists in their home community, and gain support from others in similar circumstances including gender, age, culture and other demographics that may be important to the individual. However, vulnerability is a potential risk that needs to be considered when entering the online platform.
Individuals with Serious Mental Illness represent 30% to 40% of the homeless population and as many as 25% of those same individuals have a substance dependence (Kirby & Keon, 2006). Although rural and remote homelessness in Canada remains a hidden issue, there is mounting evidence that homelessness is as prevalent in rural communities as it is in urban settings (NAERRH, 2021). As the individual with SMI moves between recovery and maintenance, the importance of housing in the stabilization of psychiatric symptoms is highlighted as a significant factor in their recovery. Stable housing is especially important for social workers to keep in mind when working in rural and remote locations where the interplay between the mezzo- and macro-levels can have a significant impact on the quality of life of the individual. This issue highlights the importance of developing a coordinated and collaborative approach encompassing all three levels of support and intervention (micro, mezzo, and macro). Social workers can provide individual support, as well as sessions for couples and families. The role of social workers in working with individuals with SMI also includes conducting psychosocial, cognitive and mental health assessments, and working as part of an interdisciplinary team to develop and support individualized treatment plans. As social workers, our work helps to reduce stigma and promote evidence-based treatment for all persons in need of support. This support may include advocacy work at the mezzo- and macro-levels to address some of the basic human needs of individuals with SMI at the municipal, provincial, and federal levels.
Maternal Mental Health
Having a baby can be an exciting and life affirming experience; however, this is not the experience of all families. The perinatal period is often an overwhelming, stressful and anxiety-inducing time that can affect every aspect of life for the woman, partner and family unit. As a social worker, working in rural and remote locations with families during the perinatal period is recognized as practice that is potentially impacted by great risk, as well as opportunity for the greatest outcomes.
In Canada, one family experiencing PMADs (Perinatal mood and anxiety disorders) is estimated to cost the healthcare system over $150,000. However, by utilizing a simple screening tool and providing access to treatment, the cost is estimated at $5000 (Bauer et al., 2014). As social workers, we also consider the hidden costs that include the impact on the child, mother, family and community. Suicide is the leading cause of death during the perinatal period for women (Bauer et al., 2014; Grigoriadis et al., 2017).
Maternal mental health is defined as “a state of well-being in which a mother realizes her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to her community” (McCauley et al., 2019, p. 2). The term perinatal refers to the period of conception up to and including 12 months after a birth. Perinatal mood and anxiety disorders (PMADs) refer to a variety of mental health issues that fall within the mental health continuum. They include Depression, Bipolar Disorder, Anxiety, Panic Disorder and Obsessive-Compulsive Disorder. In extreme situations, Psychosis can also be included, but this would be classified as a rare medical emergency.
Understanding perinatal mood and anxiety disorders (PMADs) and their origins is as complicated and unique as is the woman and family unit. As a social worker working with new or expecting families, you need to familiarize yourself with the signs and symptoms of PMADs. Risk factors increase or decrease depending on a number of factors that may include social, psychological, environmental, and hormonal issues. Families that are marginalized and experience lower socio-economic status, food insecurity, family violence, adverse life experiences, historical trauma, and are 2SLGBTQ+, are at increased risk of developing PMADs. First Nations women are 20% more likely to have post-partum depression than Caucasian women (Dharma et al., 2019). It’s important to note that not all families who share these particular factors are destined to have PMADs. However, every family is at risk of developing PMADs; for instance, even fathers/partners may experience symptoms of depression after the birth of the baby at a rate of 10% (Paulson & Bazemore, 2010).
The short- and long-term consequences of untreated perinatal mood and anxiety disorders (PMADs) can be detrimental to the woman, baby, family and community. Depression and anxiety can present distinctly for each woman, though some common features include feelings of sadness, lethargy, anger and worry. These are unlike “baby blues” that are shorter in duration and lack physical and emotional intensity. Other outcomes include impact on the partner relationship, attachment issues, as well as social, emotional and cognitive development in the baby (Letourneau et al. 2012).
When reviewing how Canada is doing with respect to maternal mental health (Hippman et al., 2022), research identified numerous gaps and regional differences, and advocates for a national perinatal mental health strategy that would target prevention and triaging into treatment and support. From a social work perspective, this advocacy work is best coordinated at all three service levels (micro, mezzo, and macro).
Parents residing in rural and remote locations are often burdened with travel costs and face the reality of having to leave their other children behind to be tended to by members of the community when they have to access labor and delivery services in larger urban centres. Some rural and remote locations may have a health centre, but due to physician shortages and the lack of locum doctors, families may be directed to another community to access care. Parents experiencing high risk pregnancies are usually directed to leave their home community at 38 weeks gestation or earlier, which can create financial barriers requiring travel and a hotel stay; the parent would then also be in an unfamiliar community without any informal supports (family and friends) to rely upon.
Building maternal mental health capacity in rural and remote locations requires a multi-faceted approach that considers the local culture, community strengths, and opportunities for development. Many remote communities have a long history of childbirth and mental wellness, and each geographic area will have its own ceremonies, traditions and protocols that honour the significance of taking care of the family in a holistic manner. The use and training of doulas and midwives who are connected to the community would be an example of building capacity at the community level, as would training of maternal mental health providers (including social workers) in a manner that is respectful of the traditions and culture of the region. Key social work competencies when working with families during the perinatal period include:
- Treating the family with respect, and honouring their specific cultural needs and requests;
- Providing education on positive mental health and appropriate screening tools;
- Sharing knowledge of both formal and informal supports available in the community to support the family unit; and
- Enhancing the attachment between baby and caregivers.
Violence
Social workers engage with vulnerable populations that are experiencing various challenges, and this includes working with survivors and perpetrators of violence. Regardless of the geographic setting, violence is a multifaceted issue and it has detrimental effects on the individual, family and community. In providing mental health supports, prevention initiatives and intervention services must consider individual, community, and societal factors and how they affect individuals and families experiencing violence. Social workers work collaboratively to initiate life-changing interventions and support mental health on a daily basis, and in rural and remote communities there is always the potential for social workers to find themselves alone in a dangerous situation during such interventions.
The World Health Organization Violence Prevention Alliance divides violence into three sub-types according to the victim-perpetrator relationship: self-directed violence (suicide, suicide attempts and self-abuse), interpersonal violence (youth violence, intimate partner violence, sexual violence, gender-based violence, child maltreatment, and elder abuse), and collective violence (violence committed by larger groups of individuals and can be subdivided into social, political and economic violence) (WHO, 2010). The World Health Organization (2010) also states that violence represents a “major health, criminal justice, human rights, and development challenge” (p. 2). It over-burdens health and mental health systems, undermines communities, and slows economic and social development (WHO, 2010).
Regardless of the type of violence that is impacting communities and mental health, social workers need to be familiar with risk assessment, risk management and safety planning. Conducting a thorough risk assessment of every client is critical, and should always include efforts to determine a prior history of violence, mental illness or other mental health-related challenges, drug and alcohol use, and weapon use. There is no doubt that information and knowledge is powerful when trying to prevent violence, and to mitigate the effects of violence.
When working in remote and rural areas, it is important to build relationships and understand the uniqueness of the community. This includes building knowledge of available resources and programs to support good mental health, and understanding cultural norms that can serve as risk factors or protective factors. Rural and remote communities do not have access to the same formal mental health supports and services as do urban centres.
Geographic isolation can contribute to barriers for those seeking services, such as a lack of transportation and limited access to appropriate resources. Other challenges for individuals who have experienced mental illness, addictions, and violence living in rural and remote areas include greater distances between homes, being less visible to neighbors or other potential witnesses, and being further away from emergency services. In many rural and remote areas there are an abundance of weapons, as well as situations where the justice system allows the return of weapons for hunting season to those charged and convicted with violent offences. Access to e-mail and the Internet, as well as adequate and consistent cell phone coverage, is not available in many areas outside of large urban centres (Kasdorff & Erb, 2010).
Rural communities have unique resources and capacities for mental health resilience such as a tightly knit network of support and a strong relationship to the natural environment (Hirsch & Cukrowicz, 2014). These can be protective factors when one fits in, and they can create a sense of belonging within close, tight-knit communities. However, these same unique resources and capacities can also contribute to a heightened risk of conflict and violence.
As a social worker delivering mental health services in areas outside of large urban centres, you will need to take proactive steps to mitigate violent encounters. First, all practicing social workers must have adequate and responsible supervision and support from a supervisor. This supervision should support ethical considerations and best practice, while instilling a culture of safety and risk reduction. Secondly, social workers should have access to relevant safety training and technology, including GPS tracking. In recent years, there have emerged a number of innovations in mental health service delivery that have the potential to be particularly helpful in rural, remote, and northern environments by creating safe options for clients and social workers outside of large urban settings.
Innovations in Mental Health Service Delivery
Telehealth is an innovation that originally emerged to help bridge the distance for residents living in rural and remote areas in order to access health care. Telehealth is defined as the use of digital information and communication technologies, such as computers and mobile devices, to access personal health care services remotely (Mayo Clinic, 2022). More specific to mental health interventions, telepsychiatry facilitates staff education and specialty consultation; reduces rural practitioners’ sense of isolation; better protects patient anonymity, potentially reduces stigma; generates reliable diagnoses; and yields high patient and provider satisfaction (Hubley et al., 2016).
In addition to more traditional telepsychiatry services, there are other options that have emerged in response to limited accessibility and resources such as telephone helplines, telephone counselling, video counselling, Internet Cognitive Behavioral Therapy (ICBT), walk-in (rapid access) counselling services, mobile apps, and other digital health platforms. The next sections will focus on mobile apps and digital health platforms, as well as walk-in counselling (rapid access) service options.
Mobile Apps and Digital Mental Health Platforms
Mental wellness/health apps and digital mental health platforms have continued to increase in popularity, and are seeing further development and growth as users download them with the hopes of managing and addressing mental health challenges and mental illness such as anxiety and depression (Marshall et al., 2020). Increasingly, governments and service providers are endorsing these options as viable alternatives to face-to-face support due to low cost, convenience, and accessibility (Parker et al., 2019). A number of treatment approaches including cognitive behaviour therapy (CBT), dialectical behaviour therapy (DBT), and prolonged exposure therapy are being assimilated into apps that can stand alone or supplement the face-to-face therapy process (East & Havard 2015).
Mental health apps and digital platforms have the potential to reach people who would otherwise not receive help by removing the barriers to access. These apps and digital platforms may reduce cost, eliminate wait-times, and may also reduce the stigma that can exist for those receiving support for mental health challenges. These support options can promote user autonomy by facilitating self-awareness and self-efficacy, which fits within the realm of social work values. For those outside of large urban centres, mental health apps may also be applied for real-time monitoring of users who are in crisis without available in-person supports (Robillard et al., 2019). Barriers to accessibility of mental health apps and digital platforms, however, exist due to connectivity issues in rural and remote locations, computer and technological literacy issues, as well as costs associated with the purchase of cell phones and computers. There is also a cost associated with accessing the apps themselves.
A lack of privacy can also pose challenges for some who do not have a private place to talk due to others in the home and/or concerns around safety. For some individuals, seeking help can risk their safety and wellbeing. As a result, there are some mental health websites and apps that have a quick exit feature to increase safety for people at risk of, or are experiencing, violence.
Finally, because there are no regulations nor standards in place for mental health apps and digital platforms, they may provide inaccurate information and resources and services that are not evidence-based; which poses ethical concerns from a social work perspective. However, these options continue to be developed and made widely available. The research and literature regarding efficacy of these approaches to support mental health and wellness is limited, but data suggests that this technology is being well-utilized by subscribed users (Marshall et al., 2020; Robillard et al., 2019).
Walk in Counselling (Rapid Access)
Walk in counselling clinics have been operating throughout Canada for over 25 years, and this approach to service delivery is more established in Canada than anywhere else in the world (Hoyt & Talmon, 2014). The rapid access model of counselling is typically implemented to help reduce barriers for individuals seeking support and as a response to diminishing resources (Harper-Jaques & Foucault, 2014). Within rural and remote communities, few affordable counselling services are often available, which can result in people not receiving help when they are seeking it. Again, this may be due to factors such as lack of transportation, length of travel time, lack of child care and/or the stigma related to seeking help. Walk in counselling services have emerged as a creative means to reduce barriers and offer individuals and families help when they need it.
Conclusion
Accessibility is one of the five pillars of the Canada Health Act (Health Canada, 2015), yet many Canadians continue to experience barriers to accessing the care that they need. This is especially true for individuals living in rural, remote, and northern areas in Canada who are seeking mental health supports and treatment options for mental illness. As service providers living and practicing in these communities outside of large urban centres, social workers are well-positioned to provide information, assessments, interventions and ongoing supports to individuals struggling with mental illness and addictions.
This chapter discussed mental health and mental illness, with a particular emphasis on the mental health continuum [MHC] model as a tool to be utilized by social workers in rural and remote settings. An exploration of enablers and barriers to accessing mental health supports was provided, and select mental health issues and challenges that social workers address in rural and remote settings was examined. In particular, suicide prevention and intervention, substance use and addictions, chronic mental illness, maternal mental health, and violence were discussed.
There continues to be stigma associated with mental illness and for those experiencing issues with their mental health. The Mental Health Commission of Canada reports that one in every five Canadians experiences a challenge to their mental health within a given year (MHCC, 2022a). While we often have a good understanding of physical illness, there tends to be less knowledge available about mental illness or substance use issues. As discussed in this chapter, a lack of understanding leads to fear and negative attitudes towards individuals living with mental illness and addictions, and it prevents people from seeking help for themselves and from providing appropriate support to people around them. These issues are even more apparent in rural and remote communities.
Just as social workers provide information, supports, and care to those in rural and remote communities who struggle with challenges to their mental health; social workers who practice in rural and remote settings must also work to maintain their own mental health and wellness. Having the support of colleagues and supervisors can be essential to avoiding burnout for any social worker. However, social workers practicing outside of large urban centres often do not find those connections easy to build. As a result, they must create supportive networks with allied professionals and social workers in different regions in order to access the feedback and collaboration that is needed for their own mental health and wellness. Maintaining good mental health is essential for good social work practice.
Nuelle Novik (pronoun she/her), a white settler who grew up in rural Saskatchewan, has lived and practiced social work in rural, remote, and urban settings. I acknowledge that my positionality grants me inherent privilege and influences the way in which I interpret the world around me.
Brent H. McKee Pronoun (He/Him); White Settler: Brent has been practicing as a Registered Social Worker in Saskatchewan within the field of mental health for over 30 years. His practice is specialized in maternal mental health and is rooted in trauma-informed practices, attachment theory and systems theory. Anti-oppressive and person-centred practices with a strong underpinning in the social determinants of health is the foundation of his work. Social work plays a pivotal role in supporting individuals, families and communities at all levels of interaction.
Karmen Pearce is a White/Caucasian female who grew up in rural Saskatchewan. She currently resides in Yorkton, SK and is employed as a Registered Social Worker.
Activities and Assignments
- Think about the various stereotypes that you have heard about people experiencing mental illness over your lifetime. Have those stereotypes changed over the years? Which of those stereotypes do you believe are still prevalent for you, or for your family, or in your community? How might these stereotypes affect you as a social worker supporting individuals and families living with mental illness in rural or remote communities?
- What are some of the barriers that individuals seeking help in order to address suicidal thoughts in rural and remote locations might encounter? What are some of the enablers that might support a suicidal individual in seeking mental health support?
- Online peer support can be beneficial for the person with serious mental illness (SMI) living outside of an urban centre. As the social worker supporting this individual utilizing online peer support, what factors would you need to consider to mitigate potential risk to the individual?
- Identify a rural or northern community that you are familiar with, and list the services that are available there to support maternal mental health. What barriers to good mental health for a family with a newborn might be present in that same community?
Additional Resources
- Mental Health Commission of Canada [MHCC]. (2021). Answering the call: Strategic plan 2021/2030. Available on the Mental Health Commission of Canada website.
References
Allport, G.W. (1937). Personality: A psychological interpretation. Holt.
American Psychiatric Association [APA]. (2021). Diagnostic and statistical manual of mental disorders (DSM-5), fifth edition. Author.
American Society of Addiction Medicine. (2019). Definition of addiction. https://www.asam.org/quality-care/definition-of-addiction
Baxter, L., Burton, A., & Fancourt, D. (2022). Community and cultural engagement for people with lived experience of mental health conditions: What are the barriers and enablers? BMC Psychology, 10(71).
Bauer, A., Parsonage, M., Knapp, M., Iemmi, V., & Adelaja, B. (2014). The costs of perinatal mental health problems. Centre for Mental Health and London School of Economics.
Brands, B., Di Ciano, P., & Mann, R.E. (2021). Cannabis, impaired driving and road safety: An overview of key questions and issues. Frontiers in Psychiatry, 12, 641549.
Canadian Association of Social Workers [CASW]. (n.d.). The role of social work in mental health.
Canadian Centre on Substance Use and Addiction [CCSA]. (2019). Canadian drug summary: Summer 2019. Author. ISBN 978-1-77178-583-9
Canadian Mental Health Association [CMHA]. (2021). Mental health and mental illness: What’s the difference? https://cmha.ca/brochure/fast-facts-about-mental-illness/
Canadian Mental Health Association [CMHA] Ontario. (2009). Backgrounder: Rural and northern community issues in mental health. https://ontario.cmha.ca/wp-content/uploads/2009/09/cmha_on_rural_northern_mental_health_issues_20090827.pdf
Canadian Mental Health Association [CMHA] Ontario. (2022). Stigma and discrimination. https://ontario.cmha.ca/documents/stigma-and-discrimination/
Chen, S.P., Chang, W.P., & Stuart, H. (2020). Self-reflection and screening mental health on Canadian campuses: Validation of the mental health continuum model. BMC Psychology, 8(76).
Chowdhury, M.R. (2021). What is the mental health continuum model? https://positivepsychology.com/mental-health-continuum-model/
Cleary, A. (2012). Suicidal action, emotional expression, and the performance of masculinities. Social Science & Medicine, 74(4), 498-505.
Creighton, G., Oliffe, J., Ogrodniczuk, J., & Frank, B. (2017). "You've gotta be that tough crust exterior man": Depression and suicide in rural-based men. Qualitative Health Research, 27(12), 1882-1891.
Dharma, C., Lefebvre, D.L., Lu, Z., Lou, W., Becker, A.B., Mandhane, P.J., Turvey, S.E., Moraes, T.J., Azad, M.B., Chen, E., Elliott, S.J., Kozyrskyj, A.L., Sears, M.R., & Subbarao, P. (2019). Risk for maternal depressive symptoms and perceived stress by ethnicities in Canada: From pregnancy through the preschool years. Canadian Journal of Psychiatry, 64(3), 190–198.
Dudley, J.R. (2000). Confronting stigma within the services system. Social Work, 45, 449-455.
Dykxhoorn, J., Hollander, A.C., Lewis, G., Dalman, C., & Kirkbride, J.B. (2019). Family networks during migration and risk of non-affective psychosis: A population-based cohort study. Schizophr Res, 208, 268-275.
East, M., & Havard, B. (2015). Mental health mobile apps: From infusion to diffusion in the mental health social system. JMIR Mental Health, 2(1).
Franken, K., Lamers, S.M.A., Ten Klooster, P.M., Bohlmeijer, E.T., & Westerhof, G.J. (2018). Validation of the Mental Health Continuum-Short Form and the dual continua model of well-being and psychopathology in an adult mental health setting. Journal of Clinical Psychology, 74, 2187–2202.
Frederick, L. (2020). Barriers to help-seeking in men for mental health issues: The impact of gender role socialization and masculine ideologies. [Master’s thesis, The City University of Seattle]. Digital Archive.
Friesen, E. (2019). The landscape of mental health services in rural Canada. UTMJ, 96(2), 47-52.
Goffman E. (1963). Stigma: Notes on the management of spoiled identity. Simon & Schuster.
Greene, K.M., Murphy, S.T., & Rossheim, M.E. (2018). Context and culture: Reasons young adults drink and drive in rural America. Accident Analysis and Prevention, 121, 194-201.
Grigoriadis, S., Wilton, A.S., Kurdyak, P.A., Rhodes, A.E., Vonder Porten E.H., Levitt, A., Cheung, A., & Vigod, S.N. (2017). Perinatal suicide in Ontario, Canada: A 15-year population-based study. CMAJ, 189(34), E1085-E1092.
Harper-Jaques, S., & Foucault, D. (2014). Walk-in single-session therapy: Client satisfaction and clinical outcomes. Journal of Systemic Therapies, 33, 29-49.
Health Canada. (2015). Canada Health Act: Annual Report (2014-2015). HC Pub: 150140.
Herek, G.M. (2002). Thinking about AIDS and stigma: A psychologist’s perspective. The Journal of Law, Medicine & Ethics, 30, 594–607.
Hippman, C.L., Adham, M., Zlobin, C., & Wong, G. (2022). An environmental scan of perinatal mental health infrastructure across Canada. Journal of obstetrics and gynaecology Canada, 44(7), 745-746.
Hirsch, J., & Cukrowicz, K. (2014). Suicide in rural areas: An updated review of the literature. Rural Mental Health, 38(2).
Hoyt, M.F., & Talmon, M. (Eds.). (2014). Capturing the moment: Single session therapy and walk-in services. Crown House Publishing Limited.
Hubley, S., Lynch. S.B., Schneck, C., Thomas, M., & Shore J. (2016). Review of key telepsychiatry outcomes. World J Psychiatry, 6(2), 269-82.
Irvine, J., & Quinn, B., (2017). Northern Saskatchewan health indicators, health status: Mortality. Athabasca Health Authority, Keewatin Yatthé Health Region and Mamawetan Churchill River Health Region. Population Health Unit, La Ronge, SK.
Jones, M.K., & Quinn, M.A. (2021). Buprenorphine–naloxone induction in the north. Can J Rural Med, 26, 35-7.
Kasdorff, D., & Erb, B. (2010). Serving victims of violence in rural communities: Challenges and best practices. Victim/Witness Assistance Program, East Region, Ontario.
Kirby, M.J., & Keon, W.J. (2006). Out of the shadows at last: Transforming mental health, mental illness and addiction services in Canada. Report of the Standing Senate Committee on Social Affairs, Science and Technology, Government of Canada.
Kitchen, P., Williams, A., & Chowhan, J. (2012). Sense of community belonging and health in Canada: A regional analysis. Social Indicators Research, 107, 103-126.
Letourneau, N.L., Dennis, C.L., Benzies, K., Duffett-Leger, L., Stewart, M., Tryphonopoulos, P.D., Este, D., & Watson, W. (2012). Postpartum depression is a family affair: Addressing the impact on mothers, fathers, and children. Issues in Mental Health Nursing, 33(7), 445-457.
Lister, K., Seale, J., & Douce, C. (2021). Mental health in distance learning: A taxonomy of barriers and enablers to student mental wellbeing. The Journal of Open, Distance and e- Learning,
MacLeod, M.L.P., Penz, K.L., Banner, D., Jahner, S., Koren, I., Thomlinson, A., Moffitt, P., & Labreque, M.L. (2022). Mental health nursing practice in rural and remote Canada: Insights from a national survey. International Journal of Mental Health Nursing, 31, 128-141.
Marshall, J.M., Dunstan, D.A., & Bartik, W. (2020). Effectiveness of using mental health mobile apps as digital antidepressants for reducing anxiety and depression: Protocol for a multiple baseline across-individuals design. JMIR Research Protocols, 9(7), e17159.
Mate, G. (2011). Close encounters with addiction. Central Recovery Press.
Mayo Clinic. (2022). Telehealth: Technology meets healthcare. Health Information. https://www.mayoclinic.org/healthy-lifestyle/consumer-health/in-depth/telehealth/art-20044878
McCauley, M., Brown, A., Ofosu, B., & van den Broek, N. (2019). “I just wish it becomes part of routine care”: Healthcare providers’ knowledge, attitudes and perceptions of screening for maternal mental health during and after pregnancy: A qualitative study. BMC Psychiatry, 19(279), 1-8.
Mental Health Commission of Canada [MHCC]. (2022a). Mental Health First Aid: Program history. https://mentalhealthcommission.ca/training/mhfa/program-history/
Mental Health Commission of Canada [MHCC]. (2022b). How alcohol and suicide are connected - a fact sheet. https://mentalhealthcommission.ca/resource/alcohol-use-and-suicide-fact-sheet/
Naslund, J., Grande, S., Aschbrenner, K., & Elwyn, G. (2014). Naturally occurring peer support through social media: The experiences of individuals with Severe Mental Illness using YouTube. PLoS ONE, 9(10), e110171.
National Alliance to End Rural and Remote Homelessness [NAERRH]. (2021). Rural & remote homelessness: A call for strategic investments in rural and remote communities across Canada.
National Institute on Drug Abuse [NIDA] (2021). Opioid overdose crisis. https://nida.nih.gov/drug-topics/opioids/opioid-overdose-crisis
NSCAD (2021). Peer mentors: Self monitoring with the mental health continuum tool. NS: NSCAD University. https://navigator.nscad.ca/wordpress/wp-content/uploads/2021/10/Mental-Health-Continuum-Tool-PDF-EDIT.pdf
Park, J., Tjepkema, M., Goedhuis, N., & Pennock, J. (2015). Avoidable mortality among First Nations adults in Canada: A cohort analysis. Health Reports, 26(8), 10-6.
Parker, L., Halter, V., Karliychuk, T., & Grundy, Q. (2019). How private is your mental health app data? An empirical study of mental health app privacy policies and practices. International Journal of Law and Psychiatry, 64, 198-204.
Paulson, J., & Bazemore, S. (2010). Prenatal and postnatal depression in fathers’ and its association with mental depression: A meta-analysis. Journal of the American Medical Association, 303(19), 1961-1969.
Perreault, S. (2019). Police-reported crime in rural and urban areas in the Canadian provinces, 2017. Juristat, Canadian Centre for Justice Statistics, 1, 3-37.
Persson, L. Dobson, K.S., & Frampton, N.M.A. (2021). Evaluation of a mental health continuum model in two samples. Canadian Journal of Behavioural Science, 54(3), 206–212.
Pijl, E.M., Alraja, A., Duff, E., Cooke, C., Dash, S., Nayak, N., Lamoureaux, J., Poulin, G., Knight, E., & Fry, B. (2022). Barriers and facilitators to opioid agonist therapy in rural and remote communities in Canada: An integrative review. Substance Abuse Treatment, Prevention, and Policy 17, 62 (2022).
Reccord, C., Power, N., Hatfield, K., Karaivanov, Y., Mulay, S., Wilson, M., & Pollock, N. (2021). Rural–urban differences in suicide mortality: An observational study in Newfoundland and Labrador, Canada. The Canadian Journal of Psychiatry, 1-11.
Robillard, J.M., Feng, T.L., Sporn, A.B., Lai, J., Lo, C., Ta, M., & Nadler, R. (2019). Availability, readability, and content of privacy policies and terms of agreements of mental health apps. Internet Interventions: The Application of Information Technology in Mental and Behavioural Health, 17, 1-8.
Schmidt, G. (2008). Professional work in remote, northern communities: A social work perspective. UNBC Community Development Institute.
Slaunwhite, A.K., & MacDonald, S. (2015). Alcohol, isolation, and access to treatment: Family physician experiences of alcohol consumption and access to health care in rural British Columbia. The Journal of Rural Health, 31(4), 335-345.
Smith, T., McNeil, K., Mitchell, R., Boyle, B., & Ries, N. (2019). A study of macro-, mezzo- and micro- barriers and enablers affecting extended scopes of practice: The case of rural nurse practitioners in Australia. BMC Nursing, 18(14), 1-12.
Statistics Canada. (2019). Health fact sheets: Heavy drinking, 2018. Author.
Steele, L.S., Durbin, A., Lin, E., Victor, J.C., Klein-Geltink, J., & Glazier, R.H. (2014). Primary care reform and service use by people with serious mental illness in Ontario. Healthcare Policy, 10(1), 31- 45.
Vakharia, S.P., & Little, J. (2017). Starting where the client is: Harm reduction guidelines for clinical social work practice. Clinical Social Work Journal, 45, 65–76.
Wang, Y., Feng, Y., Han, M., Duan, Z., Wilson, A., Fish, J., Sun, S., & Chen, R. (2021). Methods of attempted suicide and risk factors in LGBTQ+ youth. Child Abuse & Neglect, 122.
Westhues, A., Lafrance, J., & Schmidt, G. (2001). A SWOT analysis of social work education in Canada, Social Work Education, 20(1), 35-56.
World Health Organization [WHO]. (2021). WHO urges more investments, services for mental health.
World Health Organization [WHO]. (2017). Depression and other common mental disorders: Global health estimates.
World Health Organization [WHO]. (2010). Violence Prevention Alliance: Conceptual framework – November 2010. Geneva, Switzerland.
World Health Organization [WHO] (2001). World Health Report 2001. Mental health: New understanding, new hope. Geneva, Switzerland.
